Diego Pérez de Arenaza ID
Chief of Cardiovascular Imaging Section, Cardiology Service, Hospital Italiano de
Buenos Aires.
City of Buenos Aires, Argentina.
Acta Gastroenterol Latinoam 2024;54(4):296-298
Received: 27/11/2024 / Accepted: 18/12/2024 / Published
online 30/12/2024 /
https://doi.org/10.52787/agl.v54i4.453
The concept of evidence-based practice has persisted for several years and remains a cornerstone of clinical practice, representing the gold standard for optimal patient care.
The integration of artificial intelligence (AI) into evidence-based practice has the potential to revolutionize healthcare by providing more accurate diagnoses, personalized treatment plans, and improved physician-patient interactions. It is the proposed synergy between evidence-based practice and artificial intelligence.
AI encompasses the creation of machine learning technology, capable of performing high-level executive functions that normally require human intelligence. AI is emerging today not only because of programming in a neural network modality, but because the necessary substrate exists due to the exponential growth in the speed of microprocessors, as well as the enormous and growing volumes of digitized medical information.
AI can act as a second doctor in the decision-making process, where the human clinical expert can interact with the “artificial clinical expert,” leading to more accurate decisions and presenting more appropriate personalized/tailored diagnoses, prognoses and intervention plans for their patients.
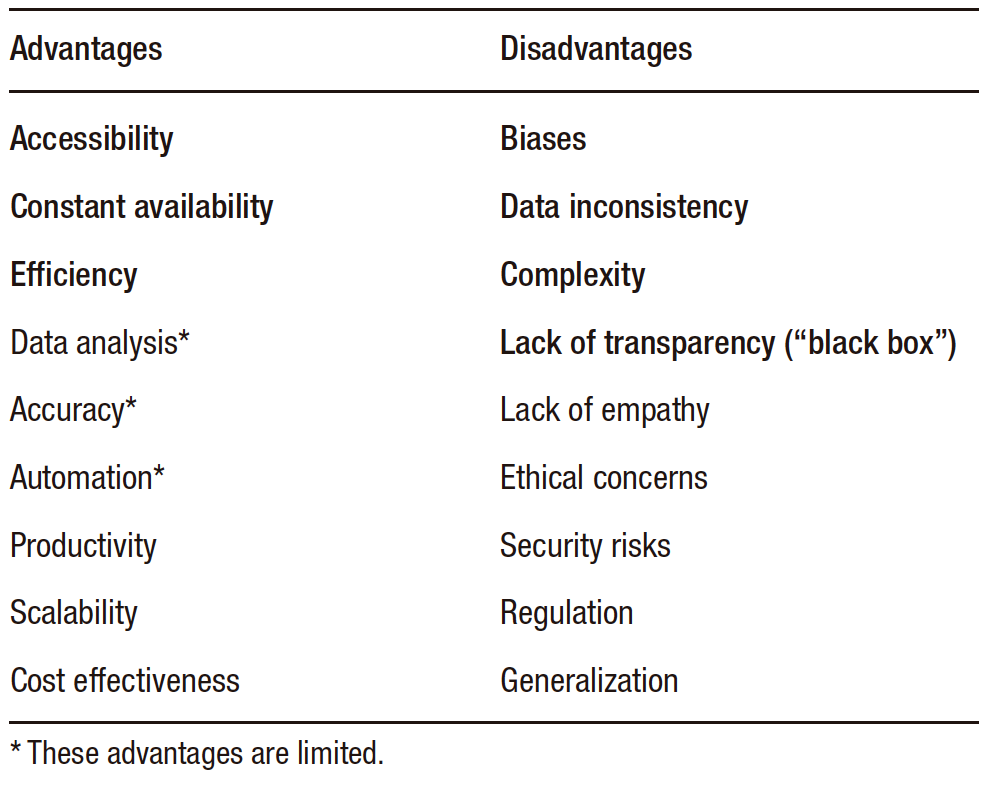
However, AI has advantages and disadvantages to consider, as listed below in Table 1.
Table 1. Advantages and Disadvantages of AI
It should be emphasized that the evidence we know today and that guides clinical guidelines and consensus is based on epidemiology and statistical analysis.
In fact, the analysis of data generated by AI (machine learning, deep learning) is not exempt from the biases of the evidence and the inconsistency of the source from which it was taken.
This applies equally to AI as it does to the evidence we deal with today. Substantially there is no radical change in how we need to evaluate these processes, to which the complexity of the technology is added.
What this “big data” generates today is a probability in relation to a myriad of data and equations that we could not perform today without this technology, but which is reduced to an estimate through Bayesian analysis, ROC curve, sensitivity analysis, multivariability (more complex processes) and associations.
AI, as complex as it may seem, uses all these types of analysis that we are already used to and, of course, estimates a probability.
That is, at one point we are estimating probabilities without assumptions (like the statistics we know), where for this reason there are still certain restrictions for the evolution of AI processes.
It is undeniable that we are all going to use this tool but let us keep in mind that it is not very far from the analysis and processes of current statistics and epidemiology, and certain problems that we are going through today with the evidence will continue (the risk estimated by these large databases cannot be generalized to other populations).
In Table 2 we refer to the basic concepts of statistics and artificial intelligence.
Table 2. Key Features of Statistical Inference and AI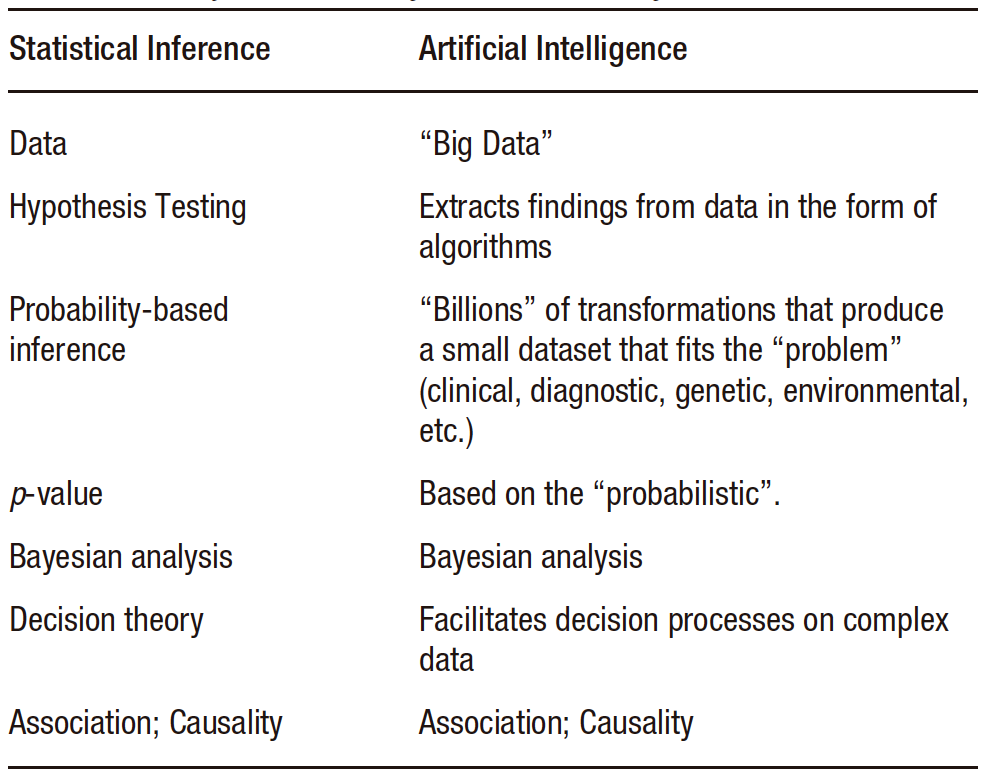
In the introduction we mentioned that AI would act as a second doctor in patient care, I would prefer to leave the doctor-patient relationship and that the contribution of technology would only serve to accentuate my critical thinking.
Critical thinking that we must not abandon, knowing the advantages of the new technology and those of traditional evidence, since in its first steps AI was based on statistical and epidemiological analysis, always associated with human intelligence.
A doctor who has critical thinking today will be better with the new tools, these will serve to enhance my expertise, someone who today only requires feedback isolated from technology will have an incomplete level of training.
AI is going to play a fundamental role in everyday life and will expand at all levels. We should be aware of its benefits and limitations so that we can act in our professional life according to the needs of the patient, either by evaluating the evidence or as a complement to medical act.
Intellectual property. The author declares that the data and tables in the manuscript are original and were carried out at his/her institution.
Funding. The autor declares that there were no external sources of funding.
Conflict of interest. The author declares that he/she has no competing interests related to this article.
Copyright

© 2024 Acta Gastroenterológica latinoamericana. This is an open-access article released under the terms of the Creative Commons Attribution (CC BY-NC-SA 4.0) license, which allows non-commercial use, distribution, and reproduction, provided the original author and source are acknowledged.
Cite this article as: Pérez de Arenaza D. Evidence in Times of Artificial Intelligence. Acta Gastroenterol Latinoam. 2024;54(4):296-298. https://doi.org/10.52787/agl.v54i4.453
Correspondence: Diego Pérez de Arenaza
Mail: diego.perezdearenaza@hospitalitaliano.org.ar
Acta Gastroenterol Latinoam 2024;54(4):296-298