Medardo Fernández-Chávez1 ID· Juliana Paiz-Tierno1 ID· Adriana Vella-Milagro1 ID· Santiago Arcentales-Peralta1
ID· Leonardo Aveiga-Cedeño1 ID· María Carolina Conlon1 ID· Renata Alina
Spiazzi1 ID· María Jimena
Cerezo1 ID· Ana
Omonte-Zambrana1 ID·
María Claudia Milano1 ID Fátima Fernández2 ID· Ricardo Gotti2
ID· Miguel
Puga-Tejada1 ID
1Gastroenterology Department, Professor Alejandro Posadas National Hospital (HNPAP); El
Palomar, Buenos Aires Province, Argentina.
2Endoscopy Department, National Hospital
Professor Alejandro Posadas (HNPAP); El Palomar, Buenos Aires Province, Argentina.
Acta Gastroenterol Latinoam 2026;56(1):86-93
Received: 21/12/2025 / Accepted: 23/03/2026 / Published online: 31/03/2026 / https://doi.org/10.52787/agl.v56i1.581
Introduction. There are different recommendations regarding the age at which colorectal cancer screening should begin using video colonoscopy (VC) in individuals under 50 years of age. Aim. To analyze the frequency of colorectal polyps in patients of any age, using data mining (DM) from a VC registry. Materials and methods. A prospective colonoscopies registry (January 2015-December 2019) was analyzed. Cases with at least one polyp were retrieved using DM, along with the characteristics of each case and polyp, and were compared according to age. Results. A total of 4,781 colonoscopies were retrieved from patients: 13.1% in those < 40 years old, 5.8% in those 40-44, 8.1% in 45-49, and 71.7% in those ≥ 50; 62.1% were female, and 62.2% were diagnostic VC. At least one polyp was identified in 15.6% of patients < 40 years old, 19.4% in those 40-44, 21.6% in those 45-49, and 34.6% in those ≥ 50 (p < 0.001). Of these, sessile serrated polyps were found in 8.2%, 5.6%, 8.4%, and 7.7%, and adenomatous polyps in 30.6%, 27.8%, 44.6%, and 49.5%, respectively. The risk of having at least one polyp increased significantly with age: 45–49 (OR 1.47; 95% CI 1.06–2.05; p = 0.02), and ≥ 50 (OR 2.81; 95% CI 2.24–3.56; p < 0.001). A minimum age of 47 years was estimated for polyps screening, and 48 years for sessile or adenomatous serrated polyps (sensitivity > 85%). Conclusion. The results of this study demonstrate a significant increase in colorectal polyps even in individuals < 50 years of age. It is necessary to evaluate colorectal cancer screening using VC at an earlier age.
Keywords. Adults, colorectal cancer, colonic polyps, video colonoscopy, young adults (source: MeSH).
Introducción. Existen distintas recomendaciones respecto de la edad de inicio del cribado de cáncer colorrectal (CCR) mediante videocolonoscopía (VCC). Objetivo. Analizar la frecuencia de pólipos colorrectales en pacientes de cualquier edad, a partir de un registro de VCC, mediante minería de datos (MD). Materiales y métodos. Se analizó un registro prospectivo de VCC (enero de 2015-diciembre de 2019). Mediante MD se recuperaron aquellos casos con al menos un pólipo, las características por caso y pólipo, y se comparó según la edad. Resultados. Se recuperaron 4781 VCC/pacientes: 13,1% en < 40 años, 5,8% en 40-44; 8,1% en 45-49 y 71,7% en ≥ 50; 62,1% femenino, 62,2% VCC diagnóstica. Se identificó al menos un pólipo en el 15,6% de los pacientes < 40 años, 19,4% en 40-44, 21,6% en 45-49 y 34,6% en ≥ 50 (p < .001). De estos, correspondieron a pólipo aserrado sésil en 8,2%, 5,6%, 8,4%, 7,7% y adenomatoso en 30,6%, 27,8%, 44,6% y 49,5%, respectivamente. El riesgo de presentar al menos un pólipo se incrementó significativamente con la edad: 45-49 (OR 1.47; IC 95% 1,06 – 2,05; p = 0,02), y ≥ 50 (OR 2,81; IC 95% 2,24 – 3,56; p < 0,001). Se estimó como mínimo una edad de 47 años para una VCC de cribado de pólipos en general, y de 48 años para aserrados sésiles o adenomatosos (sensibilidad > 85%). Conclusión. Los resultados de este estudio demuestran el incremento significativo de pólipos colorrectales aun en < 50 años. Es necesario evaluar el inicio del cribado de CCR mediante VCC a una edad más temprana.
Palabras claves. Adultos, cáncer colorrectal, pólipos colónicos, videocolonoscopía, jóvenes adultos (fuente: MeSH).
According to the American Cancer Society, colorectal cancer (CRC) screening is recommended to begin at age 45 in adults without other risk factors.1 Scientific societies in other countries maintain the recommendation to begin screening at age 50. Video colonoscopy (VC) is the gold standard for colorectal cancer (CRC) screening,2 during which colonic polyps may be found. Different follow-up protocols are used depending on the characteristics of these polyps,. Since the prevalence of CRC is much lower in adults under 50 years of age,3 in this age group, the indication for VC is based on medical judgment in response to specific clinical conditions, namely: hematochezia, anemia, constipation, chronic diarrhea, or abdominal pain.4
In these patients, the performance of colonoscopy is delayed by the performance of a battery of prior studies aimed at ruling out other clinical causes that could be responsible for these conditions.5 In order to further clarify the indication and prioritization of colonoscopy in individuals under 50 years of age, it is necessary to identify the prevalence and clinical predictors of colonic polyps and other findings on colonoscopy in this population subgroup.
There is ongoing debate regarding the age at which CRC screening should begin using VC in individuals under 50 years of age without risk factors. The evidence supporting these recommendations comes only from industrialized countries. Most studies have focused on populations under 50 years of age, without comparisons between all age groups. A significant limitation in conducting such studies lies in the retrieval, integration, and analysis of large volumes of clinical data. However, this data can be managed more efficiently through statistical programming strategies known as data mining.
The Hospital Nacional Profesor Alejandro Posadas (HNPAP) is a tertiary hospital responsible for the care of approximately four million residents in the western part of Greater Buenos Aires. It is considered a local leader in several medical specialties, including the management of various digestive diseases.
This study aims to identify the frequency of colorectal polyps using data mining from VC screening reports for patients of all ages at HNPAP. It also seeks to establish factors associated with the presence of polyps in general and adenomas/serrated polyps in particular, and, if possible, to establish an age cutoff for initiating CRC screening.
Studio design
We designed the “Polyps in Adults” Less than fifty (L in Roman numeral) years old from a Tertiary Academic Argentinian hospital” (PALTA) registry. This was a retrospective cohort observational study. Two outcomes were considered as cases: the presence of colorectal polyps in general, or adenoma/serrated polyps (explained later). The PALTA design adhered to the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines.6 Colonoscopies performed at the HNPAP and documented in a consecutively retrieved database between January 2015 and December 2019 were analyzed.
Population and sample
Inclusion criteria. Patients of any age and gender who underwent at least one VC at the HNPAP were included, regardless of the clinical context in which the procedure was requested. Since this is an observational study, cases with incomplete VC or the identification of other organic lesions (e.g., inflammatory bowel disease) alongside a pre-malignant or malignant lesion of interest to this study were not excluded.
Exclusion criteria. However, any case lacking the necessary information for the purposes of this study was excluded.
Procedure and technique
Retrieval of cases with polyps. During July 2021, a database of video colonoscopies was retrieved in MS Access format, corresponding to the study period. Using data mining, cases with at least one colorectal polyp were directly extracted. For this purpose, keywords such as “polyp” or “flat” (plano, plana) were used as a search strategy, with the respective combinations of capital letters and accents (e.g., “Pólip”, “pòlip”, “POLIP”). If relevant data such as age, date or reason for the procedure, or findings were unavailable, this information was manually retrieved from the HNPAP hospital system (SigHAP) or the physical medical record. However, if this information remained unavailable, those cases were excluded from the study.
Pathology retrieval. For patients with colorectal polyps, pathology reports were manually retrieved. These reports were then integrated into the colonoscopy database using each patient's national identity document (DNI) number. To avoid compatibility conflicts between cases with more than one colonoscopy, this integration was stratified monthly. Integrations with conflicts were resolved manually. Finally, the different histological subtypes for each case were extracted in the same way each polyp was identified, using keywords such as: “HIPERPL”, “HAMARTOMATO”, “SEUDO”, “INFLAMAT”, “ASERRAD”, etc.
Statistical analysis
Technical considerations. A p- value < 0.05 was considered statistically significant. The database was analyzed using the statistical software R v.4.0 (R Foundation for Statistical Computing ; Vienna, Austria).
Sample size estimation. A census was conducted of all cases available in the host hospital's colonoscopy database.
Data mining. This is defined as the process of analyzing large volumes of structured or unstructured data to extract useful information, identify patterns, hidden trends, and correlations. A significant volume of clinical and primary care reports was analyzed, using keywords to identify the reason for consultation and the histological endoscopic findings. The R gapminder library was used for this purpose. Primary care reports were integrated into the clinical and primary care database using the merge function.
Descriptive statistics. Quantitative variables were described as mean (standard deviation, SD) or median (interquartile range, IQR), according to their statistical distribution (Kolmogorov-Smirnov test, K-S). Qualitative variables were described as frequencies, rates, or ratios. All study variables were described according to the proposed age groups (< 40, 40–44, 45–49, and ≥ 50 years).
Inferential statistics. Multivariate logistic regression was used to establish the association between the different study variables and the identification of at least one colorectal polyp. Considering age as the numerical variable to be evaluated, and the identification of at least one colorectal polyp as the dichotomous outcome variable, the minimum age for polyp identification was estimated using a receiver operating characteristic (ROC) curve. A sub-analysis was performed for the identification of at least one adenoma.
Ethical issues
This study was approved by the Research Bioethics Committee (RBC) of the HNPAP (ref. 632LUP0S0/22). Enrolled patients signed the respective informed consent forms for clinical purposes (performance of VC). The confidentiality of patient identity and personal and clinical data was guaranteed in accordance with Law No. 25,326 on the Protection of Personal Data (Ministry of Justice and Human Rights, Republic of Argentina). The study was conducted in accordance with the Nuremberg Code of 1947 and the Declaration of Helsinki of 1964 and subsequent amendments (the latest dating from 2013).
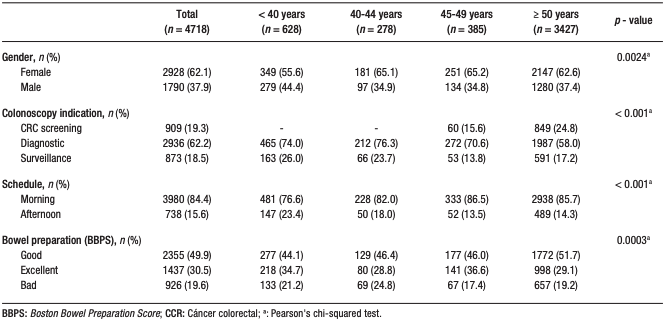
A total of 4781 colonoscopies/patients were recovered: 13.1% in patients < 40 years old, 5.8% in those 40-44, 8.1% in those 45-49, and 71.7% in those ≥ 50; 62.1% were female. The main reason for colonoscopy was diagnostic in 62.2% of cases. 80.4% of patients had good or excellent preparation. (Table 1). At least one polyp was identified in 15.6% of patients < 40 years old, 19.4% in the 40-44 age range, 21.6% in the 45-49 age range and 34.6% in those ≥ 50 years old (p < 0.001) (Figure 1).
Table 1. Characteristics of the analyzed colonoscopies, according to the proposed age
groups
Figure 1. Frequency of colorectal polyps according to the different age groups (p
< 0.001)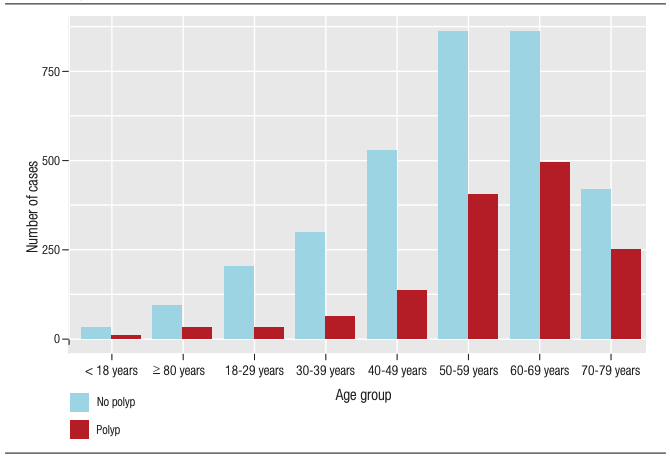
Similarly, a significantly age-related increase in the number of adenomas/serrated lesions was observed (p < 0.001) (Figure 2).
Figure 2. Frequency of adenomas or serrated lesions according to the different age
groups (p < 0.001).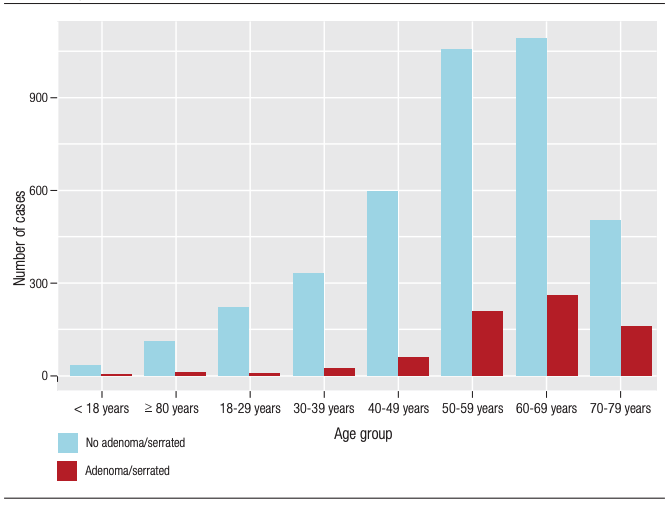
Of these, sessile serrated polyps were present in 8.2%, 5.6%, 8.4%, and 7.7%, and adenomatous polyps in 30.6%, 27.8%, 44.6%, and 49.5%, respectively (Table 2).
Table 2. Characteristics of the analyzed colorectal polyps (shape,
histology, dysplasia), according to the proposed age groups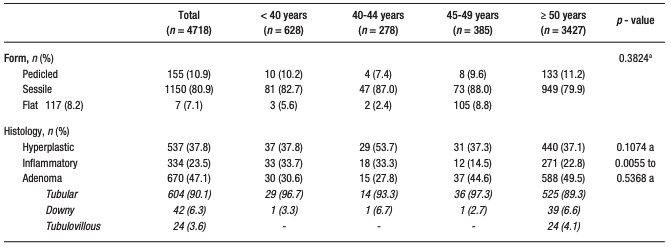
Continuation Table 2. Characteristics of the analyzed colorectal polyps
(shape, histology, dysplasia), according to the proposed age groups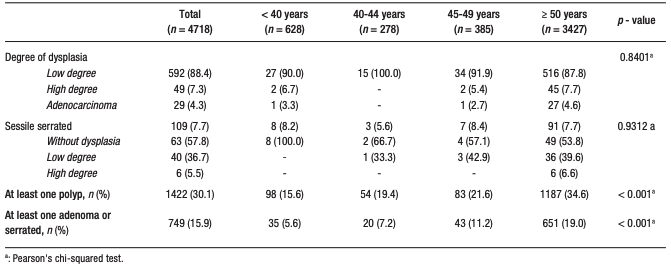
The risk of having at least one polyp increased significantly with age: 40–44 years (OR 1.37; 95% CI 0.94–1.97; p = 0.10), 45–49 (OR 1.47; 95% CI 1.06–2.05; p = 0.02), and ≥ 50 (OR 2.81; 95% CI 2.24 – 3.56; p < 0.001) (Table 3). A minimum age of 47 years was estimated for a general polyp screening, and 48 years for serrated sessile or adenomatous polyps (sensitivity > 85%).
Table 3. Multivariate logistic regression considering as outcome the identification
of at least one colorectal polyp in general, or adenoma/serrated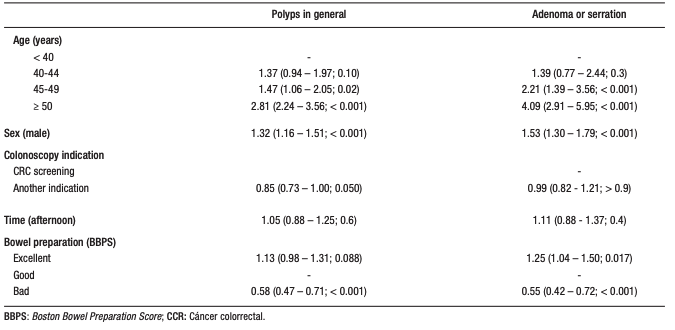
This study, which included a large cohort of 4,781 video colonoscopies analyzed using data mining, showed a significant and progressive increase in the frequency of colorectal polyps with age, with their presence even evident in patients under 50 years of age. The detection of at least one polyp was 15.6% in those under 40 years of age, increasing to 34.6% in those over 50 years of age (p < 0.001), with a similar pattern for adenomas and serrated lesions. Importantly, ROC curve analysis allowed for the estimation of an age threshold close to 47–48 years for optimizing the detection of polyps and precursor lesions, with adequate sensitivity. Taking together, these findings reinforce the significant presence of preneoplastic lesions in young individuals and provide local evidence that challenges traditional cut-off points for initiating colorectal cancer screening.
A study conducted in Alaska Natives demonstrated the presence of adenomatous polyps of varying degrees of dysplasia in 26% and 40% of cases between 40-49 and 50-59 years of age, respectively. However, the shape, location, and histology did not differ significantly between the two age groups. Considering the high frequency found in those under 50 years of age, the study concluded that screening should begin at age 40.7
However, there is also Latin American evidence on this matter. A Colombian study that considered patients aged 45-49 and 50-75 as cases and controls demonstrated a frequency of colorectal polyps of 36.7% and 42.5%, and of adenomas/serrate polyps of 18.5% and 32.4%, respectively. Similarly, it was concluded that CRC screening using visualization should begin at age 45.8
A cost-effectiveness analysis based on a Portuguese cohort from 1993 to 2010 concluded that although there is an increase in the incidence and mortality of CRC in patients between 45-55 years of age, the benefit of screening in this population would not be cost-effective unless the incidence of this neoplasm rises to 47.5 per 100,000 inhabitants, currently being 30.9
This retrospective study represents one of the few recent initiatives analyzing a large CRC screening database in Argentina. As mentioned previously, a minimum age of 47 years was estimated for CCS screening for polyps in general, and 48 years for sessile or adenomatous serrated adenomas. Although standardizing a lower age cutoff for CRC screening in a population requires more and higher-quality evidence, these results indicate the possibility of identifying polyps and adenomas in individuals under 50 years of age, while maintaining a sensitivity greater than 80%.
Strengths and limitations of the study
This study has several strengths. These include a large sample size, comparisons with patients over 50 years of age, and a clearly defined outcome in terms of polyps in general, and adenomas/serrated polyps. Among its limitations, it is worth noting that the data comes from a single hospital, rather than at a local or national level; furthermore, the database is not entirely dedicated to CRC screening. In fact, more than 80% of the cases presented with some symptom or were being monitored for a pre-existing condition. Increased identification of polyps or adenomas is possible in patients with hematochezia.10
Overcoming this technical limitation would allow for analysis of the database using the colorectal polyp as the unit of observation, nested within the colorectal volume (CCV), and this, in turn, nested within each patient. This would also allow for several sub-analyses that consider the size and location of each colorectal polyp. Finally, long-term case follow-up would enrich this type of research.
In conclusion, although the PALTA results do not describe the frequency of colorectal polyps in the general population, they do demonstrate a significant increase, even in individuals under 50 years of age, in a large hospital sample. It is suggested that the age cutoff for initiating CRC screening be reduced by two to three years. A higher identification of polyps or adenomas is significantly associated with factors such as age over 45 years, male sex, and excellent bowel preparation. Poor bowel preparation is significantly associated with a lower identification of both polyps and adenomas. It is necessary to evaluate initiating CRC screening using video colonoscopy at an earlier age.
Consent for publication. Written informed consent was obtained from the patients for participation and publication of this case.
Intellectual property. The authors declare that the data, figures and tables in this article are original and were carried out at their institutions.
Funding. The authors declare that there were no external sources of funding.
Conflict of interest. The authors declare that they have no conflicts of interest in relation to this article.
Copyright

© 2026 Acta Gastroenterológica latinoamericana. This is an open-access article released under the terms of the Creative Commons Attribution (CC BY-NC-SA 4.0) license, which allows non-commercial use, distribution, and reproduction, provided the original author and source are acknowledged.
Cite this article as: Fernández-Chávez M, Paiz-Tierno J, Vella-Milagro A et al. Frequency of Colorectal Polyps in Patiens Younger vs. Older Than Fifty Years: Analysis of 4718 Colonoscopies Through Data Mining. Acta Gastroenterol Latinoam. 2026;56(1):86-93. https://doi.org/10.52787/agl.v56i1.581
Correspondence: Miguel Puga-Tejada
Email: miguel.puga01@hotmail.com
Acta Gastroenterol Latinoam 2026;56(1):86-93