FNU Alvina1 ID· Chidera N Onwuzo1 ID· Azhar Hussain1 ID· Adaora Ojiugo Moka2 ID· Rashid Abdel Razeq3 ID· Somtochukwu Onwuzo4 ID
1Resident Physician, SUNY Upstate Medical University, Syracuse, NY-13202,
USA.
2Babcock State University: Ibadan, Oyo State,
Nigeria.
3Resident Physician, Cleveland Clinic Fairview Hospital, Cleveland, OH
44111, USA.
4Fellow Physician, Allegheny General Health, Pittsburgh, PA-15212,
USA.
Acta Gastroenterol Latinoam 2026;56(2):208-215
Received: 16/01/2026 / Accepted: 04/06/2026 / Published online: 30/06/2026 / https://doi.org/10.52787/agl.v56i2.592
Introduction. Cannabis use is increasingly prevalent among patients
with liver disease, its clinical impact on outcomes in cirrhosis remains unclear. This study evaluates
the association between cannabis use disorder and clinical complications in patients with cirrhosis.
Methods. We conducted a retrospective study using the TriNetX network. Adults aged
18-89 years with cirrhosis were divided into two cohorts: those with cannabis use disorder(n = 46,347)
and those without (n = 888,138). Propensity score matching (1:1) was performed using demographics and
key laboratory values. The final matched sample consisted of 46,168 patients in each
group.
Outcomes were assessed over a 1-year follow-up and included all-cause mortality, critical
care admission, respiratory complications, dyselectrolytemia, and hypoalbuminemia.
Results. Patients with cannabis use disorder had significantly higher odds of all-cause
mortality (OR 1.086, 95% CI 1.052-1.121), critical care admission (OR 1.400, 95% CI 1.348-1.453),
pneumonia (OR 1.212, 95% CI 1.158-1.268), pneumothorax (OR 1.160, 95% CI 1.041-1.293), and
hypoalbuminemia (OR 1.074, 95% CI 1.035-1.114). Hyponatremia (OR 1.241, 95% CI 1.191-1.293),
hyperkalemia (OR 1.102, 95% CI 1.053-1.154) and hypokalemia (OR 1.302, 95% CI 1.248-1.359) were more
frequent in the cannabis group. Non-significant associations were noted for hemothorax (OR 1.074, 95% CI
0.922-1.251) and empyema (OR 0.945, 95% CI 0.805-1.109). Conclusion. These observational findings suggest that documented cannabis use
disorder may identify a higher-risk subgroup among patients with cirrhosis, but they do not establish
causality. Clinicians may consider evaluating cannabis use when conducting risk assessment and
counseling. Further prospective research is needed to better define the mechanisms and long-term impact
of cannabis in advanced liver disease.
Keywords. Cannabis use disorder, cirrhosis, electrolyte derangement, pneumonia, ICU admission.
Introducción. El consumo de cannabis es cada vez más frecuente
entre los pacientes con enfermedad hepática, pero aun así, su impacto clínico en los resultados de la
cirrosis continúa siendo incierto. Este estudio evalúa la asociación entre el trastorno por consumo de
cannabis y las complicaciones clínicas en pacientes con cirrosis. Métodos.
Realizamos un estudio retrospectivo utilizando la red TriNetX.
El estudio incluyó a adultos de 18 a
89 años con cirrosis, divididos en dos cohortes: aquellos con trastorno por consumo de cannabis (n =
46.347) y aquellos sin él (n = 888.138). Se realizó un emparejamiento por puntuación de propensión (1:1)
en función de las características demográficas y los valores de laboratorio clave. La muestra final
emparejada estuvo compuesta por 46.168 pacientes en cada grupo. Los resultados se evaluaron durante un
seguimiento de un año e incluyeron mortalidad general, ingreso en cuidados intensivos, complicaciones
respiratorias, dislectrolitemia e hipoalbuminemia. Resultados. Los pacientes con
trastorno por consumo de cannabis presentaron una probabilidad significativamente mayor de mortalidad
general (OR 1,086; IC 95% 1,052-1,121), ingreso en cuidados intensivos (OR 1,400; IC 95% 1,348-1,453),
neumonía (OR 1,212; IC 95% 1,158-1,268), neumotórax (OR 1,160; IC 95% 1,041-1,293) e hipoalbuminemia (OR
1,074; IC 95% 1,035-1,114). La hiponatremia (OR 1,241; IC 95% 1,191-1,293), la hiperpotasemia (OR 1,102;
IC 95% 1,053-1,154) y la hipopotasemia (OR 1,302; IC 95% 1,248-1,359) fueron más frecuentes en el grupo
de consumidores de cannabis. No se observaron asociaciones significativas para el hemotórax (OR 1,074;
IC 95% 0,922-1,251) ni para el empiema (OR 0,945; IC 95% 0,805-1,109). Conclusión. Estos hallazgos observacionales sugieren que el trastorno por
consumo de cannabis documentado puede identificar un subgrupo de mayor riesgo entre los pacientes con
cirrosis, pero no establecen causalidad. Los médicos podrían considerar la evaluación del consumo de
cannabis como parte de la valoración del riesgo y la consejería clínica. Se requieren más estudios
prospectivos para definir con más exactitud los mecanismos involucrados y el impacto a largo plazo del
cannabis en la enfermedad hepática avanzada.
Palabras claves. Trastorno por consumo de cannabis, cirrosis, desequilibrio electrolítico, neumonía, ingreso en la UCI.
Cirrhosis is a chronic process characterized by fibrosis and nodule formation, leading to alteration in the normal architecture of the liver.1 Approximately 4.5 million adults in the United States were diagnosed with liver disease in 2018.2 The prevalence of cirrhosis in the United States was approximately 0.27%, corresponding to 633,323 adults with mortality rates of 21.9 per 100,000 people.3,4 The causes of cirrhosis included hepatitis C, alcohol-related liver disease, non-alcoholic fatty liver disease (NAFLD) and other conditions.5
Cannabis is the most used illicit drug in the United States, with its use increasing even in populations with cirrhosis from 2010-2021.6,7 Cannabis use disorder (CUD) as defined by ICD-10 criteria represents a clinically significant pattern of problematic cannabis use associated with impairment or distress, and does not reflect occasional or recreational consumption. Several recent preclinical studies suggest a protective effect of cannabidiol (CBD), a non-psychoactive component of cannabis, through its anti-inflammatory effects. It attenuates alcohol-induced liver steatosis, metabolic dysregulation, inflammation and neutrophil-mediated injury through the CB1 and CB2 receptors suggestive of a potential hepatoprotective role.8,9 At the epidemiological level, population studies have reported a reduced incidence of MASLD10 and alcohol-related liver disease among cannabis users.11 However, at the clinical level, particularly in patients with established cirrhosis, several studies suggest that cannabis was associated with higher rates of hepatic decompensation like ascites.12
Critically, prior clinical studies have been limited by the absence of propensity-matched designs, heterogeneous patient populations, and a failure to distinguish CUD from occasional use. Given these conflicting signals and paucity of propensity-matched data, this study fills an important evidence gap by evaluating the association between CUD and a range of clinical complications in patients with cirrhosis.
We conducted a retrospective, propensity-matched cohort study using U.S. electronic health record data from the TriNetX network, a global health research network that provides life science companies and healthcare organizations with access to de-identified patient data of over 100 million patients for clinical research and trial design.13
This retrospective cohort study included adults diagnosed with cirrhosis, using ICD-10-CM code K74.60 (unspecified cirrhosis of liver), which encompasses both compensated and decompensated presentations.
Adults aged 18-89 years with cirrhosis were divided into two cohorts: those with CUD (n = 46,347) and those without (n = 888,138).
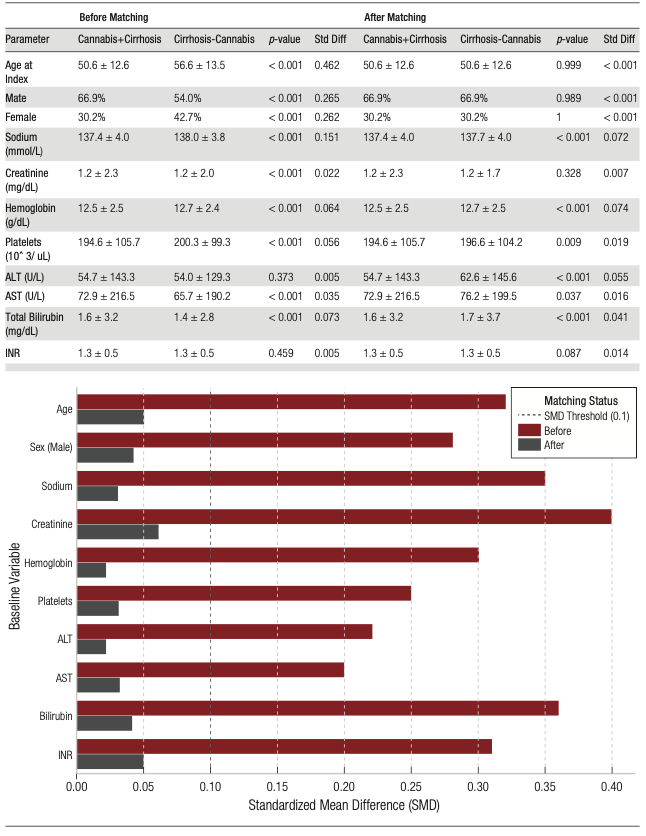
Propensity score matching (PSM) (1:1) was performed to address baseline imbalances, based on age, sex, race, common cardiovascular risk factors like hypertension and diabetes mellitus, and key laboratory values including sodium, creatinine, hemoglobin, platelets, ALT, AST, bilirubin, and INR. This was performed using a 1:1 greedy nearest neighbor matching algorithm with a caliper of 0.1 standardized mean difference to ensure precise matching. The final matched sample consisted of 46,168 patients in each group (n = 46,168).
Balance was assessed using standardized mean differences (SMDs); SMD < 0.10 was considered acceptable. Although p-values are reported for descriptive purposes, SMDs were considered the primary balance metric.
Our primary objective was to evaluate the association between CUD and 1-year outcomes among patients with cirrhosis by comparing patients with cirrhosis and CUD to those with cirrhosis but without CUD. The primary outcome was all-cause mortality; secondary outcomes included critical care admission, respiratory complications (pneumonia, pneumothorax, hemothorax, and empyema), dyselectrolytemia (hyponatremia, hyperkalemia, and hypokalemia), and hypoalbuminemia.
Statistical analysis
The analyses were conducted using TriNetX’s integrated analytical tools, which utilize R and SQL-based backend analytics within a secure cloud environment. Descriptive statistics summarized demographic and clinical characteristics, and compared between groups using the Student´s t-test or Mann-Whitney U test for continuous variables and Chi-square or Fisher’s exact test for categorical variables. Odds ratios (ORs) with 95% confidence intervals (CIs) were the primary measure of association. Kaplan-Meier survival analysis and hazard ratios (HRs) were used to assess time-to-event mortality.
Prior to PSM, the groups differed on several covariates. Among the 46,347 patients with cirrhosis and CUD (Cohort 1), patients were younger than those without CUD (50.6 ± 12.6 vs 56.6 ± 13.5 years; SMD = 0.46) and had a higher proportion of males (66.9% vs 54.0%; SMD = 0.27). Additional imbalances were observed for sodium, creatinine, platelets, AST/ALT, and bilirubin (several SMDs > 0.10; Figure 1).
Following PSM, all covariates were adequately balanced, with SMD < 0.1. Means/proportions were identical between groups: age 50.6 ± 12.6 vs 50.6 ± 12.6 years (SMD < 0.01), male sex 66.9% vs 66.9% (SMD< 0.01), sodium 137.4 ± 4.0 vs 137.7 ± 4.0 mmol/L (SMD = 0.07), creatinine 1.2 ± 2.3 vs 1.2 ± 1.7 mg/dL (SMD = 0.01), hemoglobin 12.5 ± 2.5 vs 12.7 ± 2.5 g/dL (SMD = 0.07), platelets 194.6 ± 105.7 vs 196.6 ± 104.2 ×10³/µL (SMD = 0.02), ALT 54.7 ± 143.3 vs 62.6 ± 145.6 U/L (SMD = 0.06), AST 72.9 ± 216.5 vs 76.2 ± 199.5 U/L (SMD = 0.02), total bilirubin 1.6 ± 3.2 vs 1.7 ± 3.7 mg/dL (SMD = 0.04), and INR 1.3 ± 0.5 vs 1.3 ± 0.5 (SMD = 0.01).
In the propensity-matched cohort, CUD among patients with cirrhosis associated with several complications. (Figure 2)
According to the Forest Plot, cirrhosis patients without CUD, showed significantly higher odds of all-cause mortality (OR 1.086, 95% CI 1.052-1.121), critical care admission (OR 1.400, 95% CI 1.348-1.453), pneumonia (OR 1.212, 95% CI 1.158-1.268), pneumothorax (OR 1.160, 95% CI 1.041-1.293), and hypoalbuminemia (OR 1.074, 95% CI 1.035-1.114).
Dyselectrolytemia was more frequent in the CUD group, including hyponatremia (OR 1.241, 95% CI 1.191-1.293), hyperkalemia (OR 1.102, 95% CI 1.053-1.154) and hypokalemia (OR 1.302, 95% CI 1.248-1.359).
Non-significant associations were noted for hemothorax (OR 1.074, 95% CI 0.922-1.251) and empyema (OR 0.945, 95% CI 0.805-1.109).
Figure 1. Baseline characteristics and laboratory parameters (before and after
matching)
Figure 2. Forest plot comparing odd ratios for outcomes in the
cannabis + cirrhosis vs cirrhosis without cannabis use disorder group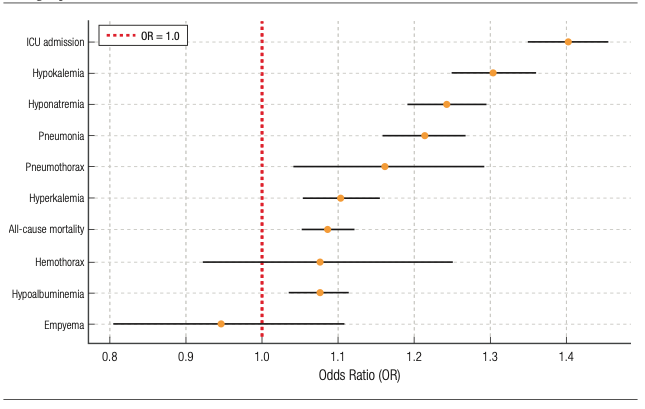
Cannabis has been legalized in over 30 states in the United States, and it is crucial to understand its effect on patients with cirrhosis.14 The endocannabinoid system has been known to play a role in cirrhosis through the CB1 and CB2 receptors which are G-protein coupled receptors.15 Within the liver, CB1 receptors have been detected in endothelial cells and hepatocytes whereas CB2 receptors have been detected in Kupffer cells and are upregulated in hepatic fibrogenic cells.16 Exocannabinoids like tetrahydrocannabinol (THC), tetrahydrocannabivarin (THCV), and CBD which are major components of cannabis act on CB1 and CB2 receptors. THC and THCV are analogs and function as CB1/CB2 agonists in high doses and a CB1/CB2 neutral antagonist in low doses. CBD functions as an indirect CB1 agonist. These could potentially increase the fibrogenic potential.17-19
Liver cirrhosis is caused by advancement in healing and fibrosis, and occurs due to chronic stimuli including viral, autoimmune, drug induced, cholestatic and metabolic diseases.20-23
Recent population studies have shown that cannabis use has significantly increased in young adults aged 26-49 years, but has remained constant in youth aged 17-25 years, with increased use noted in males as compared with females from 2021-2022.24
Prior retrospective cohort studies using the State Inpatient Database and Nationwide Inpatient Sample focused on patients with hepatitis C cirrhosis or broader cohorts with compensated and decompensated cirrhosis. In those studies, cannabis use was associated with lower mortality or morbidity among patients with alcoholic cirrhosis and other cirrhosis etiologies.25,26 In contrast, a recent meta-analysis showed that the risk of advanced liver fibrosis among HCV-infected patients who use cannabis was higher than non-users.27
Complementary to our findings, a retrospective population-based, cohort study indicated that all-cause ER visits or hospitalizations were significantly greater among cannabis users than among controls.28 Several studies indicate cannabis use is associated with longer ICU stays.29 However, there is paucity of studies specifically identifying rates of critical care admission.
Inhalation of cannabis smoke exposes to the risk of pulmonary infections including pneumonia due to the inflammation of the bronchial mucosa, leading to the alteration of the mucociliary system.30 In their cohort study, Bisconti et al. found an association between cannabis users and an increased risk of primary spontaneous pneumothorax compared with non-users.31 Similarly, another case-control study showed an increased risk of pneumothorax in exclusive cannabis users compared with exclusive tobacco smokers.32 The mechanism could be related to the higher puff volume and breath holding time which could raise intra-alveolar pressure leading to shearing force and injury.33
There is no existent literature supporting a direct causal link between cannabis use and hypoalbuminemia in healthy individuals. Firstly, albumin is a negative acute-phase reactant, and decreases during inflammatory states irrespective of hepatocyte mass, which is commonly seen in hospitalized patients.34 Secondly, cannabis exposure correlates with worse diet quality and lower BMI in the general population.35
The increased odds of dyselectrolytemia, including hyponatremia and hypokalemia, is likely related to Cannabis Hyperemesis syndrome, a term coined by Allen et al.,36 and described by Simonetti et al. in their case series37 who noted cyclical vomiting being associated with chronic cannabis use.
The increased odds of hyperkalemia noted in cannabis users with cirrhosis compared with non-users can be explained by two hypotheses. Firstly, heavy cannabis use can trigger cannabinoid hyperemesis syndrome (CHS) with severe vomiting leading to Acute Kidney Injury (AKI), diminishing distal sodium delivery and potassium excretion as described in case reports.38,39 Secondly, hyperkalemia is more plausibly explained by renal dysfunction secondary to hepatorenal physiology, the use of potassium-sparing diuretics such as spironolactone, or adrenal insufficiency, all of which are prevalent in this population.
Limitations
Although the data were obtained from a validated multicenter and research platform database of more than 70 different healthcare systems with over 130 million patients across the United States, the electronic records might have errors in timely data entry of lab values, comorbidities and even diagnosis. The absence of data on cirrhosis etiology (e.g., alcoholic, viral, metabolic) is a significant limitation, as etiology may independently influence the outcomes studied. Similarly, data on alcohol consumption, tobacco use, and opioid use, which may confound the association between CUD and complications, were unavailable for adjustment. The inability to determine the dose, frequency, or route of cannabis administration further limits mechanistic interpretation. The statistical significance observed for some outcomes (e.g., all-cause mortality OR 1.086) should be interpreted with caution given the large sample size, as small absolute differences may achieve statistical significance without corresponding clinical relevance. Finally, the observational design of the study precludes causal inference, and confounding by indication cannot be excluded.
In this large propensity-matched retrospective cohort study, CUD was associated with increased rates of all-cause mortality, critical care admission, pneumonia, pneumothorax, dyselectrolytemia, and hypoalbuminemia among patients with cirrhosis. These observational findings suggest that CUD may be a marker of increased risk in this vulnerable population, but they do not establish causality. Incorporating cannabis-use history into clinical assessment and counseling may be reasonable; however, further prospective studies are needed to determine mechanisms, clinical relevance, and long-term outcomes.
Consent for publication. Written informed consent was obtained from the patients for participation and publication of this case.
Intellectual property. The authors declare that the data and figures in this article are original and were carried out at their institutions.
Funding. The authors declare that there were no external sources of funding.
Conflict of interest. The authors declare that they have no conflicts of interest in relation to this article.
Copyright

© 2026 Acta Gastroenterológica latinoamericana. This is an open-access article released under the terms of the Creative Commons Attribution (CC BY-NC-SA 4.0) license, which allows non-commercial use, distribution, and reproduction, provided the original author and source are acknowledged.
Cite this article as: Alvina FNU, Onwuzo C N, Hussain A et al. Unmasking the Burden of Cannabis in Cirrhosis: A Propensity-Matched Real-World Analysis. Acta Gastroenterol Latinoam. 2026;56(2):208-215. https://doi.org/10.52787/agl.v56i2.604
Correspondence: FNU Alvina
Email: alvina.1898@gmail.com
Acta Gastroenterol Latinoam 2026;56(2):208-215