Fernando Cairo1 ID· Nicolás Domínguez1
ID· Andrea
Curia2 ID· Lucía
Navarro3 ID Manuel
Barbero1 ID· Ayelen
Trillo4 ID· Daniel
Calfunao5 ID· Rodrigo
Belloni4 ID· Anselmo
Adrián Bologna4 ID· Estefanía Burgos3
ID · Melina
Susana2 ID· Silvia
Mabel Borzi3 ID· Omar Andrés Galdame1
ID· Esteban
González Ballerga2 ID· Ignacio Roca1 ID
1Hospital El Cruce. Florencio Varela, Buenos Aires
Province.
2Hospital de Clínicas, José de San Martín. University of Buenos Aires,
Autonomous City of Buenos Aires.
3Hospital Interzonal General de Agudos Profesor Dr.
Rodolfo Rossi, La Plata, Buenos Aires Province.
4Hospital Interzonal General de
Agudos General José de San Martín, La Plata, Buenos Aires Province.
5Hospital
Provincial Dr. Castro Rendón, Province of Neuquén.
Argentina.
Acta Gastroenterol Latinoam 2026;56(2):185-195
Received: 05/02/2026 / Accepted: 03/06/2026 / Published online: 30/06/2026 / https://doi.org/10.52787/agl.v56i2.604
Background and aims. Many anti-HCV-positive individuals in Argentina remain lost to follow-up. We assessed a multicenter re-engagement program using complementary case-finding strategies, described the care cascade, and evaluated treatment outcomes. Methods. Five public hospitals implemented two strategies: laboratory-based screening at a tertiary hospital and its primary/secondary network, and combined medical-record/laboratory searches at four tertiary hospitals to identify prior anti-HCV positives. Lost to follow-up was operationally defined as no documented hepatology care, HCV RNA testing, or antiviral treatment within participating institutions for ≥ 12 months. A two-visit pathway was offered. Primary outcomes were re-engagement, treatment initiation, and SVR12; secondary outcomes were fibrosis stage and SVR4-SVR12 concordance. As an exploratory objective, all-cause mortality was assessed in the laboratory cohort using conditional logistic regression. Results. Across 206,053 data sources (106,917 laboratory samples; 99,136 medical records), 3,334 individuals were anti-HCV positive. After excluding cured (n = 741), deceased (n = 419), and liver-transplanted (n = 25) patients, 2,149 were potentially eligible for re-engagement; 422 (19.6%) re-engaged. Three hundred eleven (73.7%) had significant fibrosis (≥ F2 by FibroScan®). Antiviral therapy began in 224 patients: sofosbuvir/velpatasvir 70.1% and glecaprevir/pibrentasvir 29.9%. SVR12 was 97.9%; in a subset (n = 112), SVR4 showed 100% concordance with SVR12. In the laboratory cohort, anti-HCV positivity was associated with higher all-cause mortality (OR 4.75; 95% CI 3.82 - 5.94). Conclusions. Complementary case-finding plus a two-visit pathway enabled effective re-engagement and timely treatment, achieving near-universal SVR. This scalable model supports HCV micro-elimination across public hospital networks.
Keywords. Hepatitis C, patient dropouts, health services accessibility, treatment outcome, Argentina.
Introducción y objetivos. Muchas personas con serología positiva para anti-VHC en Argentina han interrumpido su seguimiento. Evaluamos un programa multicéntrico de revinculación por medio de estrategias complementarias de identificación de casos, describimos la cascada de atención y analizamos los resultados terapéuticos. Métodos. Cinco hospitales públicos implementaron dos estrategias: cribado basado en resultados de laboratorio en un hospital de tercer nivel y su red de atención primaria/secundaria, y búsquedas combinadas en historias clínicas y datos de resultados de laboratorio en cuatro hospitales de tercer nivel, a fin de identificar personas con antecedentes de resultado positivo para anti-VHC. A la interrupción del seguimiento se la definió operativamente como la ausencia de atención hepatológica documentada, determinación de ARN del VHC o tratamiento antiviral en las instituciones participantes durante ≥ 12 meses. Se ofreció un cronograma de dos visitas. Los resultados primarios fueron la revinculación, el inicio del tratamiento y la respuesta virológica sostenida a las 12 semanas (RVS12); entre los resultados secundarios se identificó el estadio de la fibrosis y la concordancia entre RVS4 y RVS12. Como objetivo exploratorio, se evaluó la mortalidad general en la cohorte, basada en resultados de laboratorio mediante regresión logística condicional. Resultados. Entre las 206.053 fuentes de datos analizadas (106.917 muestras de laboratorio y 99.136 historias clínicas), 3.334 individuos presentaron resultado positivo para anti-VHC. Tras excluir pacientes curados (n = 741), fallecidos (n = 419) y con trasplante hepático (n = 25), 2.149 fueron considerados potencialmente elegibles para la revinculación; de ellos, 422 (19,6%) se revincularon. Trescientos once (73,7%) presentaban fibrosis significativa (≥ F2 según FibroScan®). El tratamiento antiviral se inició en 224 pacientes: sofosbuvir/velpatasvir en el 70,1% y glecaprevir/pibrentasvir en el 29,9%. La RVS12 fue del 97,9 %; en un subgrupo (n = 112), la RVS4 mostró una concordancia del 100% con la RVS12. En la cohorte basada en resultados de laboratorio, la positividad para anti-VHC se asoció con una mayor mortalidad general (OR 4,75; IC 95%: 3,82 - 5,94). Conclusiones. La combinación de estrategias complementarias de identificación de casos y un cronograma de dos visitas permitió una revinculación eficaz y un tratamiento oportuno, y alcanzó las tasas casi universales de RVS. Este modelo escalable puede contribuir a la microeliminación de la hepatitis C en redes hospitalarias públicas.
Palabras claves. Hepatitis C, abandono del tratamiento, accesibilidad a los servicios médicos, resultado del tratamiento, Argentina.
Abbreviation
HCV: Hepatitis C virus.
HCC: Hepatocellular carcinoma.
DAA: Direct-acting
antiviral.
SVR: Sustained virologic response.
SVR12: Sustained
virologic response at 12 weeks post-treatment.
SVR4: Sustained virologic response at
4 weeks post-treatment.
LTC: Linkage to care.
EHR: Electronic health
record.
MAFLD: Metabolic dysfunction-associated fatty liver
disease.
PCR: Polymerase chain reaction.
FIB-4: Fibrosis
index-4.
APRI: AST to platelet ratio index.
WHO: World Health
Organization.
LSM: Liver stiffness measurement.
● Two-visit pathway achieved 19.6% re-engagement and 97.9% SVR12 across five public hospitals in Argentina.
● Median time to treatment was 29 days in real-world public settings.
● Complementary lab and record-based searches identified missed HCV cases.
● Genotype 1 predominated (≈ 41%), consistent with regional epidemiology.
Chronic hepatitis C virus (HCV) infection remains a major global health burden, with an estimated 58 million people chronically infected worldwide and approximately 290,000 HCV-related deaths annually, mostly due to HCC.1 The advent of DAAs has transformed the therapeutic landscape, enabling SVR rates above 95% across all genotypes and patient populations, even in real-world settings.2-4 As a result, WHO has proposed an ambitious plan to eliminate viral hepatitis as a public health threat by 2030, with specific goals including a 90% reduction in new infections, 65% reduction in related mortality, and 80% treatment coverage of eligible individuals.5
However, despite these therapeutic advances, major gaps persist along the continuum of care. Globally, fewer than 30% of infected individuals are aware of their diagnosis, and only a fraction of those have initiated treatment.6 These gaps are particularly evident in low- and middle-income countries, where healthcare systems face structural fragmentation, limited integration of services, and barriers to continuity of care. Argentina reflects this global trend, with universal access to DAAs through public programs but suboptimal diagnosis rates, fragmented data systems, and insufficient strategies to ensure linkage to care.7
The care cascade for HCV includes several steps-screening, diagnosis, linkage, staging, treatment, and follow-up-each of which is vulnerable to patient attrition. While population-based screening programs and laboratory notifications improve early identification, LTC remains the critical bottleneck in many settings.8 Patients may be lost at any point, particularly between detection of anti-HCV antibodies and confirmatory RNA testing, or between diagnosis and clinical staging.9,10 Studies from Latin America have described high rates of loss to follow-up and delays in evaluation, especially among patients from vulnerable populations or those without clear navigation systems.11,12
To overcome these challenges, targeted re-engagement programs have been proposed. These initiatives focus on identifying individuals with prior HCV diagnosis who remain untreated, often using centralized EHR, laboratory databases, or chart reviews.13-15 In high-income countries, re-linkage efforts have demonstrated success in improving access to treatment and achieving SVR in marginalized populations.16,17 However, evidence from low- and middle-income countries remains limited, and the implementation of such programs in fragmented systems like Argentina’s poses unique logistical and structural barriers.18,19
Beyond logistical challenges, individual-level factors also affect care continuity. Patients may be unaware of their infection, underestimate disease severity, or remain skeptical of treatment efficacy. A recent study in Argentina reported that more than 60% of patients identified with chronic HCV had not accessed specialist care, and a significant proportion were unaware of curative treatment availability.20 These findings support the development of structured, proactive strategies that integrate clinical data with active outreach to maximize re-engagement.
This study aims to evaluate the effectiveness of a multicenter re-linkage to care program for HCV patients in Argentina. By leveraging large-scale laboratory datasets and implementing coordinated re-engagement strategies across five high-complexity public hospitals, we assessed patient identification, clinical staging, treatment initiation, and SVR outcomes. The findings provide critical insights for future micro-elimination efforts in middle-income countries facing healthcare fragmentation and high disease burden.
1. Study design and setting
We conducted a dual-phase multicenter cohort study-retrospective identification of eligible cases followed by a prospective re-engagement and follow-up phase-at five tertiary-level hospitals in Argentina: Hospital El Cruce (Florencio Varela), Hospital José de San Martín (La Plata), Hospital de Clínicas José de San Martín (Buenos Aires), Hospital Castro Rendón (Neuquén) and Hospital Rossi (La Plata).
For the retrospective component (1 January 2013-31 December 2023), we screened electronic laboratory registers and medical records to identify patients with documented anti-HCV antibody positivity or detectable HCV RNA who were no longer receiving specialist care.
During the prospective phase (January 2024–June 2025), the cohort thus identified was contacted by telephone, invited to attend a hepatology visit, underwent clinical re-evaluation, and, when appropriate, started on DAA therapy. Patients were subsequently followed through assessment of SVR12.
2. Patient identification strategies
Two distinct strategies were implemented to identify eligible patients, depending on the institution:
• Combined record- and laboratory-based strategy: implemented at Hospital de Clínicas José de San Martín and subsequently adopted by Hospital José de San Martín, Hospital Castro Rendón, and Hospital Rossi. This approach combined targeted queries of each site's laboratory information systems (e.g., anti-HCV and HCV RNA), with focused review of medical records labeled “Hepatitis C”, whether handwritten or electronic, depending on the local format, following the model described by Sotera et al.20 Patients were considered eligible if they were ≥ 18 years old, had no documented hepatology care, HCV RNA testing, or antiviral treatment within the participating institutions during the previous 12 months, and met at least one of the following criteria:
(1) positive anti-HCV serology;
(2) detectable HCV RNA without prior antiviral treatment;
(3) prior antiviral treatment without documented SVR.
Anti-HCV positivity was used as a broad initial identification criterion to maximize case retrieval across fragmented data systems. Therefore, the eligible denominator should be interpreted as a population potentially requiring reassessment and re-engagement in care, rather than as a cohort with confirmed active infection. Re-engagement was assessed as a programmatic outcome, whereas treatment initiation and virologic outcomes were evaluated subsequently among patients who completed confirmatory assessment and, when appropriate, initiated antiviral therapy.
• Laboratory-based strategy: Hospital El Cruce employed a laboratory-driven approach. We queried institutional laboratory databases for all anti-HCV chemiluminescent immunoassays (CLIA/CMIA) performed between 2013 and 2023. Adults (≥ 18 years) with reactive results (signal-to-cutoff > 1.0), and no recorded SVR were flagged. Patients with documented SVR, death, or liver transplantation were excluded through cross-referencing with clinical and administrative databases.
This dual-strategy design enabled comparison between combined medical record and laboratory screening, and large-scale automated laboratory surveillance. Exclusion criteria-SVR achievement, death, or liver transplantation -were applied to both identification strategies to ensure comparability.
3. Standardized re-engagement protocol
Regardless of the identification strategy, all centers applied a shared, structured three-step protocol for clinical re-engagement:
Step 1 - Telephone contact: patients were contacted using the most recent phone numbers available in hospital records, with up to three call attempts made at different times and on different days. Those who could be reached were classified into one of the following categories: eligible and willing to attend follow-up, already receiving care at another institution, declined further follow-up, deceased, or liver transplant recipients.
Step 2 – Outpatient evaluation: eligible patients were scheduled for an in-person hepatology evaluation, which included a directed medical history, physical examination, and updated laboratory testing. When prior HCV RNA status was unknown, a reflex testing algorithm was applied, consisting of anti-HCV retesting followed, if reactive, by HCV RNA quantification and genotyping using real-time PCR. Liver stiffness was assessed in all patients by transient elastography (FibroScan, Echosens, Paris, France). Liver Stiffness Measurement was categorized using the following cutoffs: F0 - F1 (< 7.0 kPa), F2 (7.0- 9.4 kPa), F3 (9.5-12.4 kPa), and F4 (≥ 12.5 kPa). Significant fibrosis was defined as ≥ F2 according to elastography findings.
Step 3 – Clinical resolution and treatment: Liver fibrosis staging was performed using the best available method (APRI, FIB-4, elastography, liver biopsy, or clinical indicators such as signs of portal hypertension). Antiviral treatment was prescribed through national or provincial health programs. Follow-up continued until SVR12 confirmation.
Patients who achieved SVR12 and had mild fibrosis (F1-F2) were referred to general medical care. Those with advanced fibrosis or comorbid liver conditions (e.g., MAFLD, alcohol-related liver disease, iron overload) remained under hepatology follow-up.
4. Data collection and variables
Demographic, clinical, and virologic data were collected from available sources for the overall cohort and were completed during re-evaluation for patients who returned to care. These variables included age, sex, HCV genotype, fibrosis stage, awareness of diagnosis and treatment options, antiviral regimens initiated, and treatment outcomes (SVR4 and SVR12). Data were retrieved from patient interviews, hospital electronic and paper records, and laboratory databases, with confirmatory testing performed at national reference laboratories.
5. Outcomes
Re-engagement was defined as return to specialist care with completion of baseline staging (clinical assessment, HCV RNA testing, and FibroScan), regardless of current HCV RNA status. The re-engagement rate was calculated as the proportion of eligible anti-HCV-positive individuals (n = 2,149) who were re-engaged. Accordingly, this denominator reflects anti-HCV-positive individuals potentially eligible for reassessment within the participating systems and should not be interpreted as a cohort with confirmed viremic infection. Primary outcomes were (i) the proportion of re-engaged patients who initiated DAA therapy and (ii) SVR12 among those who initiated therapy. Secondary outcomes included (i) the re-engagement rate among eligible patients; (ii) time from first outbound contact to the first DAA dose (days, median, IQR); (iii) in-person visit burden before treatment initiation (number of visits); (iv) concordance between SVR4 and SVR12 among patients with both assessments (percent agreement); and (v) strategy-specific performance (laboratory-based vs. combined record- and laboratory-based) for re-engagement, treatment initiation, SVR12, and time-to-treatment. Additionally, all-cause mortality in the laboratory-based cohort was assessed as a pre-specified exploratory analysis.
6. Exploratory mortality analysis
We constructed a matched cohort restricted to the laboratory-identified population at Hospital El Cruce. Each anti-HCV-positive individual was matched to up to two anti-HCV-negative controls based on sex, age, and sample origin. Because some cases lacked two eligible matches, the final average case-to-control ratio was 1:1.5 (range, 1:1 - 1:2). The endpoint was all-cause mortality, ascertained through linkage with national death registries. The index date was defined as the qualifying laboratory test. Because the timing of HCV diagnosis and follow-up initiation was heterogeneous and could not be uniformly determined, mortality was evaluated as a binary outcome rather than as a time-to-event endpoint.
7. Statistical analysis
Categorical variables were summarized as n (%) and continuous variables as median (IQR). Group comparisons used χ² or Fisher’s exact tests for proportions and the Wilcoxon rank-sum test for continuous variables, as appropriate. All tests were two-sided, and p < 0.05 was considered statistically significant. We report 95% CIs for key proportions using the Wilson method. SVR4-SVR12 concordance was summarized as percent agreement among patients with both assessments. For the strategy comparison (laboratory-based vs. combined), we contrasted re-engagement, treatment initiation, SVR12, and time-to-treatment using the tests described above.
For the matched mortality analysis, the association between anti-HCV positivity and all-cause mortality was estimated using conditional logistic regression with a stratum for each matched set, with up to two matched controls per case based on sex, age, and sample origin. As a robustness check, we fitted an unconditional logistic regression model adjusted for the same covariates, with standard errors clustered by matched set. Missing data were handled using a complete-case analysis.
Analyses were performed in R 4.2.1 (R Foundation for Statistical Computing).
8. Ethical statements
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki (and its later amendments) and received prior approval from the Institutional Review Boards (Research Ethics Committees) of all participating centers (coordinating IRB: Comité de Ética en Investigación, Hospital de Alta Complejidad en Red El Cruce Néstor Kirchner, Florencio Varela, Buenos Aires, Argentina; approval letter dated May 14, 2024). For the retrospective data extraction -considered minimal risk and based on de-identified records - the IRBs waived written informed consent. For the prospective re-engagement, follow-up, and treatment phase, verbal informed consent was obtained at first contact. This consent modality was approved by the coordinating Ethics Committee (Comité de Ética en Investigación, Hospital El Cruce Néstor Kirchner, Florencio Varela, Buenos Aires, Argentina; approval letter dated May 14, 2024), which reviewed and endorsed the full study protocol including consent procedures.
1. Screening and eligibility
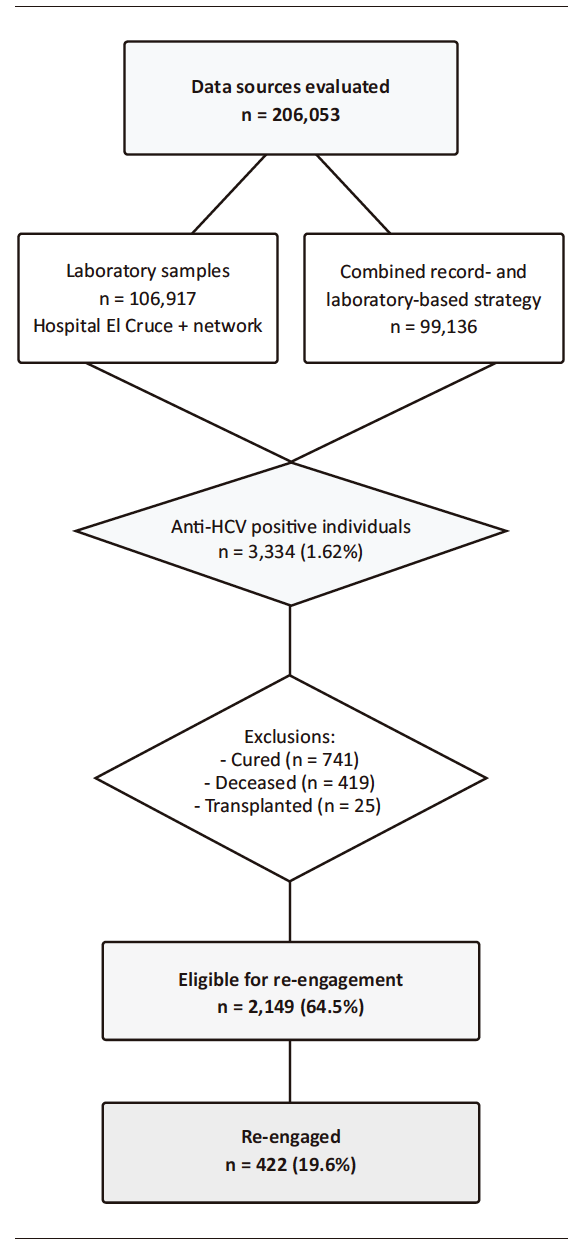
Between March and November 2024, a total of 206,053 data sources were evaluated, comprising 99,136 patient records screened using a combined query of institutional medical record systems and laboratory databases at four intermediate–high level hospitals in Argentina, and 106,917 laboratory samples processed at Hospital El Cruce, originating both from the hospital itself and from its associated network of low-complexity peripheral healthcare centers (Figure 1: Flowchart).
Figure 1. Flowchart
In total, 3,334 unique individuals (1.62%) were identified as anti-HCV positive across both strategies. The laboratory-based strategy flagged 1,162 individuals and the combined record- and laboratory-based strategy 1,330; because some individuals appeared in both sources, these counts are not additive. After excluding those already cured (n = 741), deceased (n = 419), or previously transplanted (n = 25), 2,149 patients remained potentially eligible for re-engagement. This denominator should not be interpreted as representing confirmed active HCV infection, since some anti-HCV- positive individuals may have spontaneously cleared infection or received treatment outside the participating systems. This group represented 64.5% of all anti-HCV-positive individuals and approximately 1.04% of the total population screened.
Positivity rates varied across healthcare settings. In primary care facilities within the Hospital El Cruce network, 89,009 tests were conducted, with a positivity rate of 0.43%. In hospitals of intermediate-high complexity, 100,071 tests were performed, yielding a positivity rate of 2.19%. Meanwhile, in high-complexity tertiary hospitals -including centers involved in organ, cell, and tissue transplantation-, 16,973 tests were conducted, with the highest positivity rate observed at 4.34% (Figure 2).
2. Re-engagement and staging
Among eligible patients, 422 (19.6%) were successfully re-engaged in care. 124 (29.4%) were identified through the laboratory-based approach at Hospital El Cruce and 298 (70.6%) through the combined record- and laboratory-based strategy at the other participating tertiary centers. Among those re-engaged, 311 (73.7%) had significant liver fibrosis (≥ F2) as assessed by FibroScan®.
Patient awareness assessment revealed that 15% were unaware of their HCV-positive status, 10% did not know that effective treatments existed, and 64% were unaware of the risk of disease progression.
Genotype data were available for most re-engaged patients, revealing a predominance of genotype 1, which accounted for 40.99% of cases when combining subtypes 1a (22.00%) and 1b (18.99%). Other identified genotypes included genotype 3 (18.72%), genotype 2 (8.24%), and genotype 4 (8.13%), while 24.92% of cases were either not genotyped or genotyping was not performed.
Figure 2. Anti-HCV positivity by healthcare level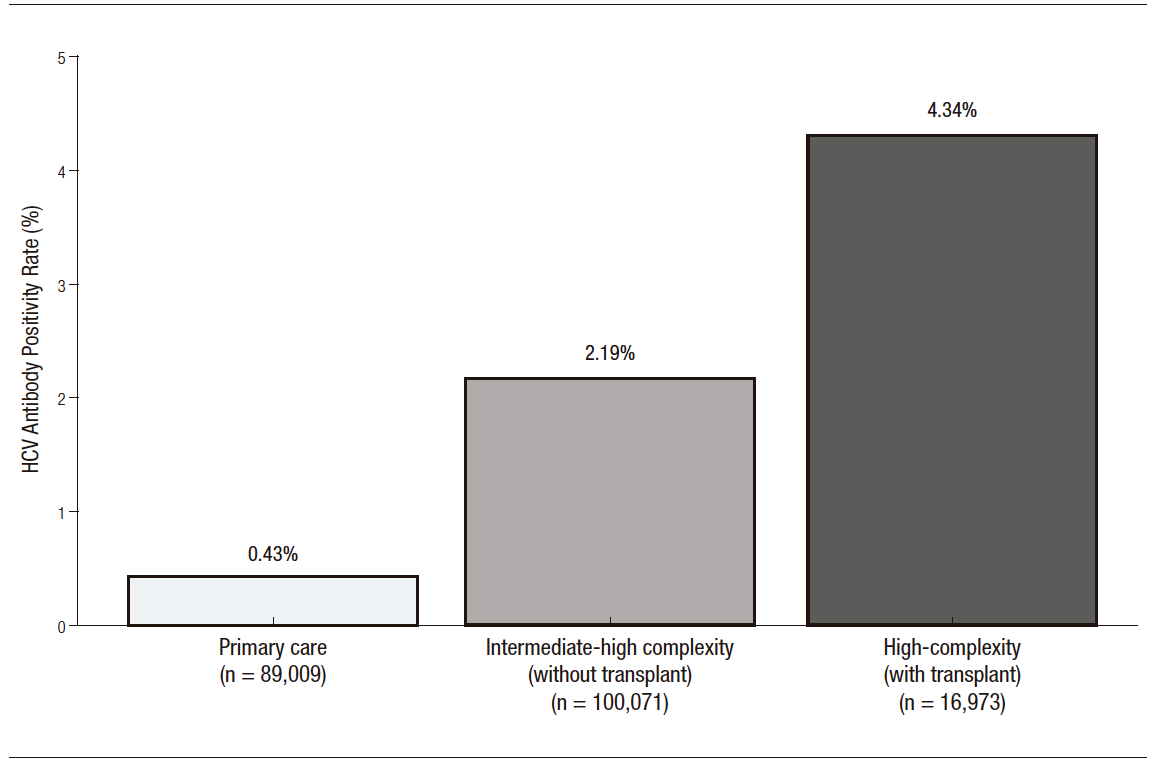
3. Treatment and virologic outcomes
Among 422 patients re-engaged in care, 224 (53.1%) initiated antiviral therapy -86 from the laboratory-based strategy and 138 from the combined record- and laboratory-based strategy. Two pangenotypic regimens were used: sofosbuvir/velpatasvir (n = 157; 70.1%) and glecaprevir/pibrentasvir (n = 67; 29.9%). The overall SVR12 rate was 97.9%; no statistically significant difference was detected between sofosbuvir/velpatasvir (98.1%) and glecaprevir/pibrentasvir (97.0%; p = 0.74). Among a subset of 112 patients, SVR4 was also assessed and showed 100% concordance with SVR12, reinforcing its usefulness as an early predictor of SVR.
4. Time-to-treatment and visit burden
The simplified pathway reduced the median time from first successful outbound contact to first DAA dose to 29 days, requiring only two in-person clinic visits to treatment start. These operational metrics were consistent across participating centers and did not materially differ by identification strategy.
5. Strategy comparison
Using a laboratory-based strategy at Hospital El Cruce, 106,917 laboratory samples were analyzed, leading to the identification of 1,162 anti-HCV positive cases (1.09%). Among these, 124 patients (10.7%) were successfully re-engaged in care, and 86 patients (69.4% of those re-engaged) initiated antiviral treatment.
In parallel, applying a combined record- and laboratory-based strategy at four intermediate- and high-complexity hospitals, 99,136 clinical records were queried against institutional medical record systems and laboratory databases, resulting in the identification of 1,330 anti-HCV-positive individuals (1.34%). Among those identified, 298 patients (22.4%) were successfully re-engaged in care, and 138 patients (46.3% of those re-engaged) initiated antiviral treatment (Figure 3).
Figure 3. Outcomes of re-engagement and treatment initiation in laboratory-based vs.
combined record- and laboratory-based strategies
6. Mortality analysis
In an exploratory analysis restricted to the Hospital El Cruce laboratory-based cohort, anti-HCV-positive status was associated with higher all-cause mortality compared with matched anti-HCV-negative controls (OR 4.75; 95% CI, 3.82–5.94; p < 0.001). Matching yielded an average case-to-control ratio of 1:1.5 (range, 1:1-1:2), with balance across the matching variables (Figure 4).
Figure 4. Association between anti-HCV antibody positivity and overall mortality,
stratified by sex, age, and site of sample origin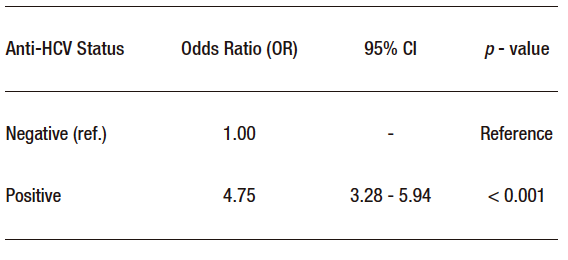
This multicenter re-engagement initiative successfully identified and treated patients with chronic HCV who had been lost to follow-up, particularly during the COVID-19 pandemic. By applying a systematic methodology across five high-complexity centers in Argentina, including one center with a solid organ transplant unit (Hospital El Cruce), the program achieved a 19.6% re-engagement rate from the eligible population. Remarkably, Hospital El Cruce also contributed the full dataset from associated low-complexity peripheral centers, broadening the scope of screening across healthcare levels. Among re-engaged patients, 73.7% presented with advanced fibrosis (≥ F2), reflecting the ongoing challenge of delayed diagnosis and underscoring the critical need for timely intervention in high-risk populations.
Previous studies have documented the impact of the COVID-19 pandemic on the continuity of care for chronic liver disease patients, with nearly half of HCV-infected individuals in some institutions lacking follow-up even before the pandemic.20 Our re-engagement yield (19.6%; 422/2,149) compares favorably with national retrieval initiatives such as the Netherlands CELINE programme14,15 which leveraged linkage of laboratory and registry data to identify and re-contact HCV-positive individuals. Differences in methodology and health system structure may account for this discrepancy, as our approach incorporated targeted phone outreach, dedicated clinic days, and coordination with public health authorities to streamline care.
Our findings should be interpreted within the broader framework of HCV micro-elimination initiatives. Similar retrieval strategies in the Netherlands, Brazil, and Taiwan have shown that active search of previously diagnosed individuals can improve linkage to care and treatment uptake.12-15 However, many of those initiatives were implemented in settings with more integrated laboratory, registry, or clinical information systems than those currently available in the Argentine public sector.18,19 In contrast, our study was conducted in a fragmented middle-income public healthcare setting, where incomplete interoperability, variable record quality, and decentralized treatment pathways represent substantial barriers. Therefore, the value of our results lies not only in the re-engagement achieved, but also in showing that a pragmatic strategy based on complementary data sources and simplified evaluation can be implemented under constrained real-world conditions. At the same time, the overall re-engagement rate indicates that retrieval alone is insufficient to close the HCV care gap, and that broader micro-elimination efforts in Argentina will likely require more integrated registries, reflex testing pathways, and patient-navigation strategies.12-15,18,19
A key success of the intervention was the significant reduction in time from initial contact to treatment initiation. Traditionally, accessing DAAs in our center required approximately six consultations and could take two to six months. However, under this program, treatment was initiated in just two visits, with a median delay of 29 days. This was achieved through multiple strategies, including telephone consultations, simplified diagnostic workflows, and partnership with the Ministry of Health to expedite medication delivery -an approach aligned with global recommendations for simplified care models.5,10,17
Among re-engaged patients, 224 initiated treatment (overall 53.1% [224/422]; 69.4% in the laboratory-based group [86/124] and 46.3% in the combined group [138/298]), and SVR12 was achieved in 97.9% of those who completed follow-up. Furthermore, SVR4 and SVR12 correlated perfectly in the subset of patients assessed for both, highlighting the potential utility of early viral response as a reliable predictor of cure, especially in resource-limited settings.4
Both re-engagement strategies -laboratory-based and combined record- and laboratory-based- proved effective in identifying and linking previously lost-to-follow-up patients to care. Each method offered distinct operational advantages. Laboratory-based screening facilitated higher specificity and more accurate contact tracing, while the review of clinical records enabled broader identification of past cases across institutional registries. The choice of strategy should be adapted to local infrastructure, availability of structured data, and integration with existing healthcare networks. In settings with centralized laboratory databases, automated queries may optimize outreach. Conversely, institutions with robust clinical documentation systems may benefit from combined medical-record audits and laboratory database queries.
Importantly, a large proportion of patients were unaware of their HCV diagnosis (15%), of available curative treatments (10%), or of disease progression (64%), consistent with prior reports from Argentina that show persistent gaps in awareness and access to care.20,21 These findings reinforce the need for public education and proactive case-finding strategies to complement biomedical efforts toward elimination.
Many cirrhotic patients in our cohort had previously documented mild fibrosis. However, heterogeneity in staging tools and follow-up intervals across centers precludes deriving a reliable average progression time; therefore, we did not model fibrosis progression.
A further limitation is that anti-HCV positivity was used as the initial screening criterion to maximize case retrieval across fragmented data systems. Consequently, the eligible denominator may overestimate the true burden of active infection, since some individuals may have spontaneously cleared HCV or received antiviral treatment outside the participating systems.
Loss to follow-up was defined operationally within the participating institutions. Therefore, some individuals classified as disengaged may have continued care or received treatment in other healthcare settings not captured by the available databases, which may have introduced non-differential misclassification.
We were unable to perform a robust multivariable analysis of predictors of re-engagement because several clinically relevant variables, particularly fibrosis stage and HCV genotype, were only available or were completed during post-retrieval evaluation and were therefore not systematically available for individuals who did not return to care. In addition, baseline data were not uniformly available across participating centers.
Despite favorable outcomes, the program faced several challenges. The absence of electronic health records slowed data collection and limited follow-up analysis, particularly regarding causes of death in non-eligible patients. Additionally, 5.5% of contacted individuals declined further care, and 4.2% did not attend the scheduled visit, likely due to socioeconomic barriers exacerbated by the pandemic, barriers also described in earlier studies on linkage-to-care efforts in Latin America.7,9
The mortality analysis should be interpreted as exploratory and center-specific, as it was restricted to the laboratory-based cohort from Hospital El Cruce, where linkage with mortality registries was feasible. Due to heterogeneity in data structure, follow-up timing, and ascertainment across participating institutions, this finding cannot be generalized to the entire multicenter cohort. Although the observed association is consistent with previous literature, in the context of our study it should be interpreted with caution and not considered a generalizable estimate for the full multicenter cohort.
In conclusion, both laboratory-based and combined record- and laboratory-based re-engagement strategies proved effective in identifying and treating patients with chronic HCV who had been lost to follow-up. The choice between approaches should be context-specific, taking into account available data infrastructure, institutional capacity, and integration with public health systems. These findings support the implementation of pragmatic re-engagement strategies as part of broader HCV micro-elimination efforts in fragmented public healthcare settings.
CRediT authorship contribution statement
Fernando Cairo (Hospital El Cruce): conceptualization, methodology, project administration, writing -original draft, supervision, formal analysis, funding acquisition, visualization.
Nicolás Domínguez (Hospital El Cruce): data curation, investigation, project administration, writing -review & editing.
Lucía Navarro (Hospital El Cruce / Hospital Rossi): data collection, investigation, resources, validation.
Manuel Barbero (Hospital El Cruce): data curation, investigation, formal analysis.
Omar Andrés Galdame (Hospital El Cruce): investigation, resources, writing -review & editing. Ayelén Trillo (HIGA San Martín): investigation, resources, data curation.
Daniel Calfunao (Hospital Castro Rendón): investigation, resources.
Rodrigo Belloni (HIGA San Martín): supervision (site), investigation, project administration.
Adrián Bologna (HIGA San Martín): data curation, validation.
Estefanía Burgos (Hospital Rossi): data collection.
Andrea Curia (Hospital de Clínicas): site coordination, investigation.
Melina Susana (Hospital de Clínicas): data collection, investigation.
Silvia Mabel Borzi (Hospital Rossi): supervision (site), investigation, project coordination.
Esteban González Ballerga (Hospital de Clínicas): methodology, supervision, writing -review & editing.
Ignacio Roca (Hospital El Cruce): statistical analysis, methodology, writing -review & editing, supervision.
Consent for publication. Written informed consent was obtained from the patient or, where applicable, from the patient's parent, legal guardian, or family member for the publication of clinical data and/or images for scientific purposes. A copy of the signed consent form is available for review by the editors of this journal.
Intellectual property. The authors declare that the data and figures presented in this manuscript are original and were generated at their respective affiliated institutions.
Funding. This study was funded by a research grant from Gilead Sciences awarded to Fernando Cairo. The funding source had no role in the study design, data collection, data analysis, data interpretation, or the writing of the manuscript.
Conflict of interest. Fernando Cairo received a research grant from Gilead Sciences. The remaining authors declare no competing interests.
Copyright

© 2026 Acta Gastroenterológica latinoamericana. This is an open-access article released under the terms of the Creative Commons Attribution (CC BY-NC-SA 4.0) license, which allows non-commercial use, distribution, and reproduction, provided the original author and source are acknowledged.
Cite this article as: Cairo F, Domínguez N, Curia A et al. Re-engagement of Hepatitis C Patients Lost to Follow-Up: A Multicenter Study from Argentina. Acta Gastroenterol Latinoam. 2026;56(2):185-195. https://doi.org/10.52787/agl.v56i2.604
Correspondence: Fernando Cairo
Email: fernando.cairo@hospitalelcruce.org
Acta Gastroenterol Latinoam 2026;56(2):185-195