C V Noejovich1,2 ID· N Bhola3 · J J Blom2,3 ID· M P Temprano4 ID· D Armstrong1,2,3 ID· M I Pinto-Sanchez1,2,3 ID
1McMaster University, Hamilton, ON, L8S 4K1, Canada.
2Farncombe Family Digestive Health Research Institute, Hamilton, ON, L8S 4K1,
Canada.
3Hamilton Health Sciences, Hamilton, ON, L8S 4K1, Canada.
4Fundación Favaloro, Buenos Aires, Argentina.
Acta Gastroenterol Latinoam 2026;56(2):154-172
Received: 21/05/2026 / Accepted: 19/06/2026 / Published online: 30/06/2026 / https://doi.org/10.52787/agl.v56i2.653
Celiac disease requires strict adherence to a gluten-free diet, which can significantly affect eating behaviors and increase the risk of eating disorders and disordered eating. Although clinically challenging, distinguishing between these conditions is essential in the context of prescribed dietary restrictions. In this literature review, we identified an increased risk of eating disorders, particularly anorexia nervosa, in individuals with celiac disease, as well as disordered eating behaviors, including excessive restriction, food-related anxiety, and social avoidance, all of which are associated with reduced quality of life. However, current assessment tools do not adequately distinguish between pathological eating behaviors and appropriate adherence to a prescribed therapeutic diet. Although a multidisciplinary approach that includes nutritional and mental health support is recommended, evidence-based therapeutic strategies specific to celiac disease are still lacking. Overall, eating disorders in celiac disease are common and clinically relevant, highlighting the need to improve their detection and develop more appropriate diagnostic tools for both clinical practice and research.
Keywords. Celiac disease, eating disorders, disordered eating, gluten-free diet, anorexia nervosa, avoidant/restrictive food intake disorder.
La enfermedad celíaca requiere una adherencia estricta a la dieta libre de gluten, lo que puede afectar significativamente las conductas alimentarias y aumentar el riesgo de trastornos de la conducta alimentaria y alimentación desordenada. Si bien resulta clínicamente desafiante, diferenciar estas entidades es fundamental en el contexto de una restricción dietética prescrita. En esta revisión de la literatura, identificamos un mayor riesgo de trastornos de la conducta alimentaria , especialmente de anorexia nerviosa, en personas con enfermedad celíaca, así como conductas de alimentación desordenada, incluyendo restricción excesiva, ansiedad relacionada con los alimentos y evitación social, todas asociadas con una menor calidad de vida. Sin embargo, las herramientas de evaluación actuales no distinguen adecuadamente entre conductas alimentarias patológicas y la adherencia adecuada a una dieta terapéutica prescrita. Aunque se recomienda un abordaje multidisciplinario que incluya apoyo nutricional y de salud mental, aún faltan estrategias terapéuticas específicas basadas en evidencia para la enfermedad. En conjunto, la patología alimentaria en la enfermedad celíaca es frecuente y clínicamente relevante, lo que resalta la necesidad de mejorar su detección y desarrollar herramientas diagnósticas más apropiadas tanto para la práctica clínica como para la investigación.
Palabras claves. Enfermedad celíaca, trastornos de la conducta alimentaria, alimentación desordenada, dieta libre de gluten, anorexia nerviosa, trastorno evitativo/restrictivo de la ingesta alimentaria.
Celiac disease (CeD) is a chronic, immune-mediated condition triggered by gluten -the primary protein complex found in wheat, barley, and rye- that develops in genetically susceptible individuals.1 It is one of the most common digestive disorders worldwide and affects approximately 1% of the world's population.2
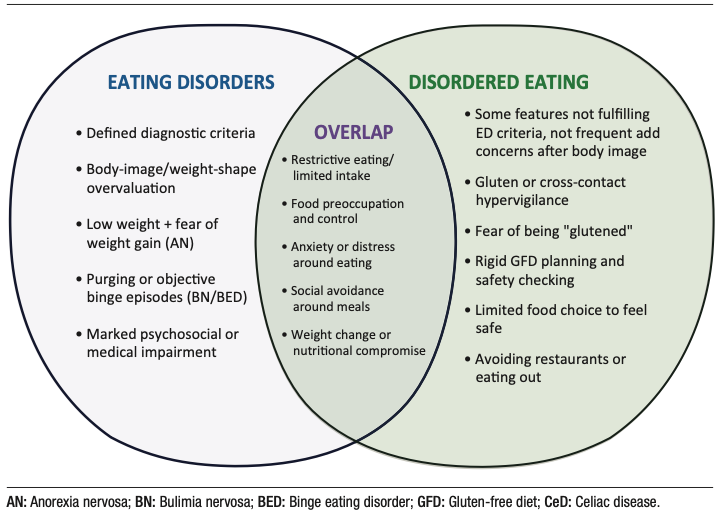
Treatment of CeD requires strict and lifelong adherence to a gluten-free diet (GFD), as even minimal exposure to gluten can trigger an immune response.This dietary restriction represents a sustained burden for patients; their relationship with food, eating behaviors, and food-related anxiety are key factors in treatment adherence and long-term clinical outcomes.3 The constant vigilance required to maintain adherence to the GFD may contribute to the development of eating behavior disturbances,4 including disordered eating (DE). This phenomenon must be distinguished from eating disorders (EDs), clinically defined psychiatric conditions that generally precede a diagnosis of CeD or arise from psychological, social, or environmental factors independent of this disease. (Figure 1).
Figure 1. Similarities and Differences Between Eating Disorders and Disordered
Eating
EDs are psychiatric conditions characterized by persistent disturbances in eating behaviors and associated thoughts, with significant medical consequences and psychosocial impairment. The main diagnostic categories include anorexia nervosa (AN), bulimia nervosa (BN), binge-eating disorder (BED), and avoidant/restrictive food intake disorder (ARFID).5 In contrast, DE represents a spectrum of maladaptive food-related attitudes and behaviors, such as rigid dietary restriction, fasting, skipping meals, or binge eating. Although these behaviors do not meet full diagnostic criteria for an ED, they may be associated with psychological distress, nutritional compromise, and suboptimal medical management.6,7 This distinction is particularly relevant in gastrointestinal conditions such as CeD, inflammatory bowel disease (IBD), irritable bowel syndrome (IBS) and food allergies or intolerance, where medically indicated dietary restrictions may evolve into excessively restrictive eating patterns or maladaptive eating behaviors.6,7
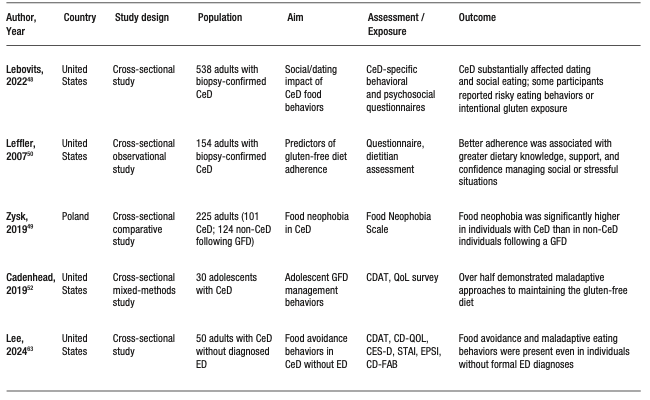
This review summarizes the current literature on ED and DE in individuals with CeD (Table 1 and Table 2), with the aim of guiding clinical recommendations and identifying critical knowledge gaps for future research.
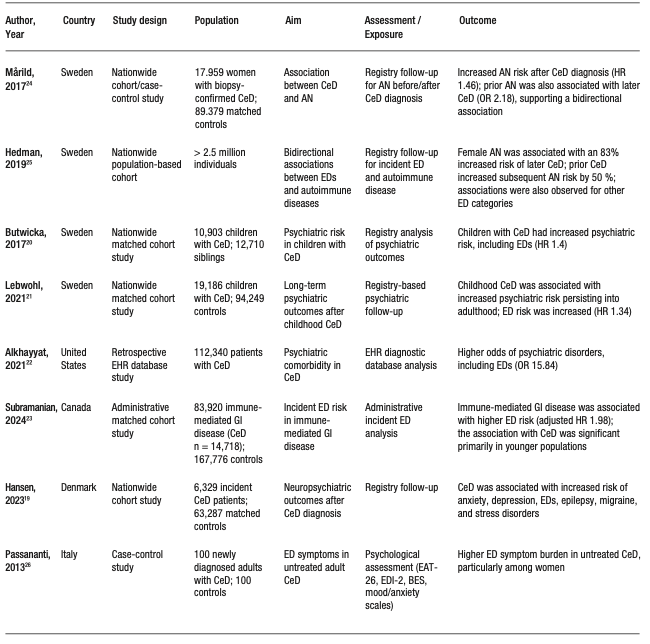
Table 1. Studies on Eating Disorders in Celiac Disease
Continuation Table 1. Studies on Eating Disorders in Celiac Disease
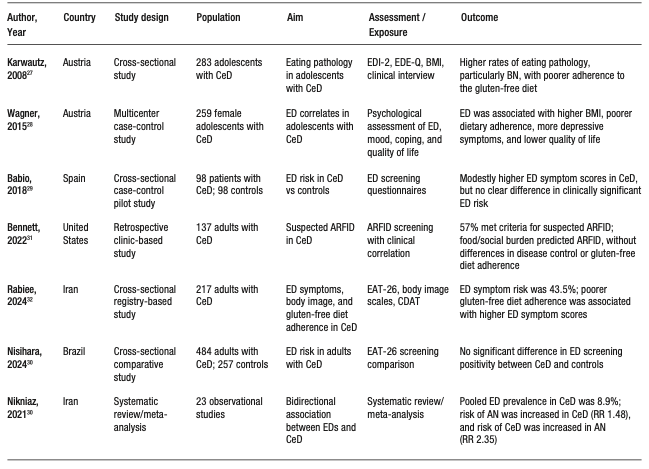
Table 2. Studies on Disordered Eating in Celiac Disease
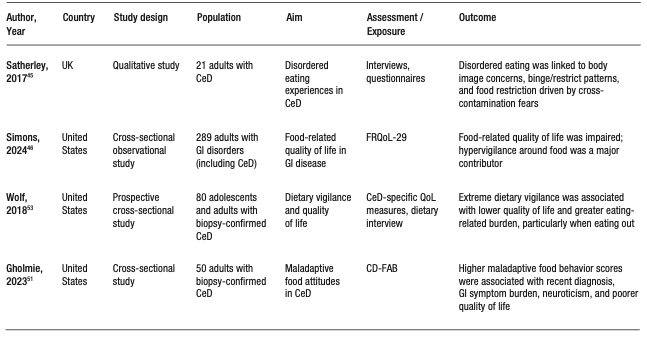
Continuation Table 2. Studies on Disordered Eating in Celiac Disease
Eating Disorders
Eating disorders (ED) are serious psychiatric conditions characterized by persistent disturbances in eating behavior and associated thoughts or emotions, leading to significant impairment of physical and psychosocial health.8,9 The estimated lifetime prevalence of ED is approximately 1 in 7 males and 1 in 5 females by age 40, with 95% of incident cases occurring before age 25.10
This review focuses on anorexia nervosa (AN), bulimia nervosa (BN), binge eating disorder (BED), and avoidant/restrictive food intake disorder (ARFID), as this are the diagnoses most frequently addressed in research and clinical practice related to CeD (Table 3).
Anorexia nervosa (AN) is characterized by persistent restriction of energy intake leading to significantly low body weight, an intense fear of weight gain, and disturbances in body image perception, often accompanied by poor insight into illness severity and behaviors that interfere with weight restoration.8 AN includes two subtypes: the restricting type and a binge-eating/purging type, the latter involving recurrent episodes of binge eating and/or purging in addition to severe restriction.8 Complications are multisystemic, with frequent gastrointestinal involvement.11 They are accompanied by significant cognitive and emotional disturbances, high medical morbidity, and psychiatric comorbidity.8 Recent global estimates place the point prevalence of AN at approximately 43.9 cases per 100,000 individuals (0.04%) in the general population.8 Onset typically occurs in early or middle adolescence, is more common in females, and generally has a more favorable prognosis in adolescents than in adults.12 Notably, AN is associated with one of the highest mortality rates among psychiatric disorders.13
Bulimia nervosa (BN) is characterized by recurrent binge eating episodes, defined as the consumption of an objectively large amount of food accompanied by a sense of loss of control, followed by inappropriate compensatory behaviors intended to prevent weight gain, such as self-induced vomiting, misuse of laxatives, fasting, or excessive exercise.8 To meet diagnostic criteria, these behaviors must occur at least once a week over a three-months period, and self-evaluating must be disproportionately influenced by body shape and weight. When the individual has a significantly low weight, the diagnosis is reclassified as anorexia nervosa, binge-purge subtype.13 Recent estimates report a global prevalence of BN of approximately 156.85 cases per 100,000 individuals (0.16%) in the general population.14
Table 3. Most Common Eating Disorders Diagnoses in Celiac Disease and Main
Symptoms75-76
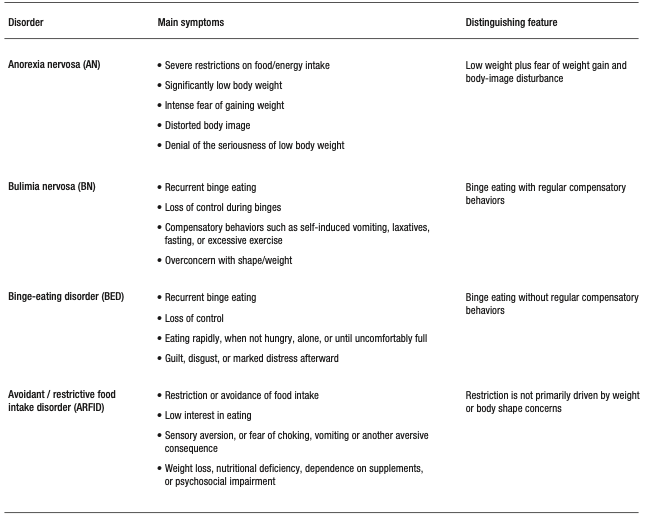
Binge-eating disorder (BED) is characterized by recurrent episodes of binge eating without compensatory behaviors, occurring at least once a week for a minimum of three months.8 These episodes typically involve the rapid consumption of large quantities of food, eating in the absence of hunger, eating until a feeling of uncomfortably fullness is reached, and marked emotional distress, including feelings of shame, guilt, or depression.13 BED is approximately twice as common in women as in men and represents the most prevalent eating disorder. Its estimated global prevalence is 1.9%, reaching 2.6% in the United States, and it accounts for approximately 47% of all ED diagnoses.15,16
Avoidant/restrictive food intake disorder (ARFID) is an eating disorder characterized by persistent avoidance or restriction of food intake that leads to an inability to meet nutritional requirements. It has clinically significant consequences, including weight loss, nutritional deficiencies, dependence on supplements or nutritional support therapies, and psychosocial impairment, in the absence of body image or weight concerns.8 ARFID may manifest as highly selective eating, low appetite, sensory-based food avoidance, or restriction driven by anxiety or fear of adverse consequences, such as choking or vomiting.13 ARFID differs from disordered eating (DE), a term describing problematic eating behaviors or attitudes, such as food avoidance or dietary restriction, that may be transient or context-dependent and do not necessarily result in clinically significant nutritional, functional, or psychosocial impairment.
Population-based data from the United States indicate that individuals with eating disorders defined according to DSM-5 criteria -including AN, BN, BED and ARFID- have higher rates of concurrent psychiatric comorbidity, particularly mood disorders, anxiety disorders, substance use disorders, and personality disorders. Among these comorbidities, major depressive disorder is the most common, followed by alcohol use disorder.17
Table 3 summarizes the most common eating disorders in celiac disease
Eating Disorders in Celiac Disease
The association between eating disorders (ED) and celiac disease (CeD) varies across available studies. A meta-analysis and systematic review18 reported a combined prevalence of EDs of 8.88% in individuals with CeD, and identified a bidirectional relationship between the two conditions, with the strongest and most consistent association observed with anorexia nervosa (AN). Population-based studies, in both adult19 and pediatric cohorts20 have also demonstrated an increased risk of ED in individuals with CeD. Similarly, Lebwohl et al.21 reported an elevated risk of ED both before and after CeD diagnosis, supporting a complex bidirectional temporal relationship. Furthermore, large studies based on administrative database from the United States and Ontario suggest that individuals with CeD have a modest to substantially increased risk of ED diagnoses compared with controls, with reported increases of approximately 1.5 to 2 times, depending on the population studied and the ED subtype.22,23
Population-based cohort studies provide more specific evidence regarding the bidirectional association between CeD and AN. A Swedish national study showed that individuals with biopsy-confirmed CeD had an approximately 1.4 to 1.5 fold higher risk of developing AN compared to the general population. Conversely, individuals with a prior diagnosis of AN had an approximately 2-fold higher risk of subsequently developing CeD.24 These findings have been replicated by Hedman et al.,25reinforcing the consistency of the epidemiological link between CeD and AN.
The clinical presentation of ED in CeD is highly heterogeneous. In adults with
untreated CeD, higher scores on measures of eating disorder symptoms have been reported,
particularly in
women, with Eating Attitudes Test (EAT-26) scores that are approximately 1.5 to 2 times
higher than
those observed in controls.26
In adolescents, higher rates of BN and a broader spectrum of eating disorders have been
described
(between 10 and 15% in some cohorts), with CeD preceding the onset of ED in most
cases.27 In
adolescents with CeD, the presence of comorbid EDs was associated with higher BMI, more
depressive symptoms,
and poorer quality of life compared to those without EDs.28 The association with a
higher BMI
suggests that disordered eating in this population are not limited to restrictive phenotypes
with
low-weight.
However, findings from case-control studies remain inconsistent. For instance, Babio et al.29 reported only modest differences in screening scores for EDs between individuals with CeD and controls, while Nisihara et al.30 found no significant difference in ED risk. More recently, ARFID has emerged as a clinically relevant phenotype in CeD, with one study reporting that more than half of adults with CeD met criteria suggestive of ARFID,31 driven primarily by food-related anxiety and social burden associated with eating.
The relationship between DE and GFD adherence also appears complex. Although one might expect restrictive phenotypes such as AN or ARFID to be associated with greater dietary rigidity and higher adherence to the GFD, Rabiee et al.,32 found that higher scores on symptoms consistent with EDs were significantly associated with lower adherence to the GFD.
Taken together, these findings suggest a higher burden of ED symptoms in subgroups of individuals with CeD, although estimates vary substantially depending on study design, the population assessed, and the measurement methods used. The most consistent evidence supports a bidirectional relationship between CeD and AN, whereas associations with other ED subtypes remain less robust.
Diagnosis and Assessment of Eating Disorders in Celiac Disease
The diagnosis of ED is primarily clinical and should be based on DSM-5-TR criteria rather than on screening instruments.8 Although ED can occur across all ages, gender, or ethnic background, adolescents and young adults are the groups at highest risk, and AN typically presents at an earlier age than BN.33
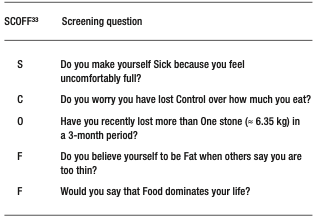
A comprehensive assessment should include evaluation of weight changes over time, patterns of food restriction or binge eating, the use of compensatory behaviors (Table 3), and attitudes associated with eating and body image, along with screening for psychiatric and medical comorbidities.8,9 The evaluation should also consider the patient’s motivation for treatment and the availability of psychosocial support.12 Brief screening tools such as the SCOFF (Table 4),34 can be useful as a first step; however, a positive result requires confirmatory diagnostic evaluation by a mental health professional, ideally a psychiatrist.13,35 Diagnostic confirmation can be supported by structured interviews such as the Eating Disorder Examination (EDE)36 and the Eating Disorder Assessment for DSM-5 (EDA-5).37 Similarly, self-administered instruments such as the Eating Disorder Inventory (EDI-3)38 can be useful for monitoring symptoms and conducting longitudinal assessment.39 Given the potential for medical instability associated with EDs, including bradycardia, hypotension, electrolyte disturbances, dehydration, or signs of malnutrition, medical risk should be systematically evaluated when an ED is suspected, with referral to higher-level care when clinically indicated.13,40
Table 4. SCOFF34 Screening of Eating Disorders in Clinical
Practice
Clinical Management of Eating Disorders in Celiac Disease
The management of EDs in individuals with CeD requires a dual approach, integrating strict medical treatment of CeD with evidence-based therapeutic interventions for EDs. This overlap poses significant clinical challenges, as adherence to the GFD may inadvertently reinforce restrictive or obsessive eating patterns. Consequently, care should be provided by an integrated multidisciplinary team, with the goal of ensuring consistent messaging, minimizing unnecessary food-related fears, and clearly differentiating between medically indicated dietary restrictions and pathological restrictive behaviors driven by the ED.
As with patients without CeD, effective management of ED in CeD relies on a coordinated multidisciplinary approach, with individualized treatment based on the patient’s specific diagnosis, age, nutritional status, and medical risk. Collaboration among physicians, dietitians, and mental health professionals is essential, and early diagnosis, along with timely, evidence-based intervention, is associated with better clinical outcomes.9,13,40 In BED, the primary therapeutic goals include nutritional rehabilitation and weight restoration, combined with disorder-specific psychotherapy; in adolescents and young adults with family or caregiver support, family-based treatment is the strategy of choice.9,12,40 Cognitive-behavioral therapy (CBT) is the first-line treatment for BN, and fluoxetine may be considered as an adjunctive treatment or effective therapeutic alternative when clinically indicated.35,40 In AN, behavioral therapy (BT) and interpersonal psychotherapy have demonstrated solid efficacy, in both individual and group formats, and antidepressants may be considered in selected cases.35,40 The management of ARFID focuses on restoring adequate nutritional intake, correcting nutritional deficiencies, expanding diet variety, and addressing avoidance behaviors through behavioral interventions, exposure-based therapies, cognitive-behavioral therapy, and family-based treatments.41,42 The evidence for ARFID treatment remains more limited than for other EDs, and there is currently no universally accepted standard approach. In general, a stepped-care and coordinated model is recommended, in which treatment intensity is adjusted to the level of clinical risk, simultaneously integrating medical, nutritional, and psychological support.35,40,42,43
Disordered Eating in Celiac Disease
In CeD, strict adherence to the GFD introduces unique challenges that can significantly influence eating behaviors.4,44-46 The need for constant vigilance -including careful review of food labels, prevention of crosscontact, and management of social situations involving food- can lead to increased monitoring of food intake and food-related anxiety.4,47 Although these behaviors are adaptive and medically necessary, in some individuals they evolve into maladaptive patterns resembling DE, such as excessive restriction, behavioral rigidity, or avoidance of eating outside the home.46,48-51 Emerging evidence suggests a complex interaction between CeD and DE behaviors, with potential implications for psychological well-being and quality of life. It has been demonstrated that individuals with CeD exhibit higher rates of food neophobia, compared with non-CeD individuals -defined as fear or avoidance of new or unfamiliar foods-and of orthorexia nervosa (ON), characterized by a pathological preoccupation with consuming foods perceived as healthy, pure or “clean”. These situations involve restrictive dietary behaviors, food avoidance, emotional distress when these behaviors are violated, and potential nutritional or psychosocial impairment.49 In CeD, the distinction between AN and ON can be challenging, given that medically appropriate gluten avoidance may resemble orthorexic behaviors; clinical concern arises when dietary restriction becomes excessive, anxiety-driven, nutritionally harmful, or extends beyond what is medically necessary. Satherley et al.45 reported elevated DE symptom scores in CeD populations, including both restrictive behaviors and episodes of binge eating. Similarly, Cadenhead et al.,52 found that more than half of adolescents with CeD exhibited maladaptive eating patterns, such as rigidity, excessive preoccupation with food, and food avoidance, which were associated with a reduced quality of life.
Dietary vigilance itself appears to contribute to disease burden. Adaptive
vigilance
in maintaining a GFD involves proportionate and flexible behaviors that support safe disease
management,
whereas hypervigilance is characterized by excessive, anxiety-driven monitoring that leads to
unnecessary
restrictions, social impairment or a reduced quality of life. Studies on various
gastrointestinal diseases,
including CeD, have shown that strict dietary control is associated with increased food-related
hypervigilance and reduced food-related quality of life.46-48
In specific CeD cohorts,51-53 greater adherence to the GFD has been associated with a
greater
perceived burden and lower quality of life, while maladaptive food attitudes assessed using
tools such as
the Celiac Disease Food Attitudes and Behaviors (CD-FAB) scale correlated with less
favorable
patient-reported outcomes.
The social implications of GFD adherence further exacerbate this burden. Lebovits et al.48 reported that 68.4% of CeD patients indicated a moderate-to-major impact of their diagnosis on dating life, including concerns about physical intimacy and discomfort when discussing dietary needs in public settings, which contributed to episodes of intentional nonadherence. Similarly, Leffler et al.50 found that adherence to a GFD negatively affected social functioning, with 44.2% of participants avoiding eating outside the home and 21.4% avoiding participation in social events. These factors may contribute to both intentional non-adherence and the development or maintenance of maladaptive eating behaviors.
Overall, current evidence suggests that, while dietary vigilance is essential for
CeD
management, it may also predispose a subgroup of individuals to the development of DE behaviors,
with
important implications for psychological well-being and quality of life.
Table 3 summarizes studies on DE behaviors in CeD.
Diagnosis and Assessment of Disordered Eating in Celiac Disease
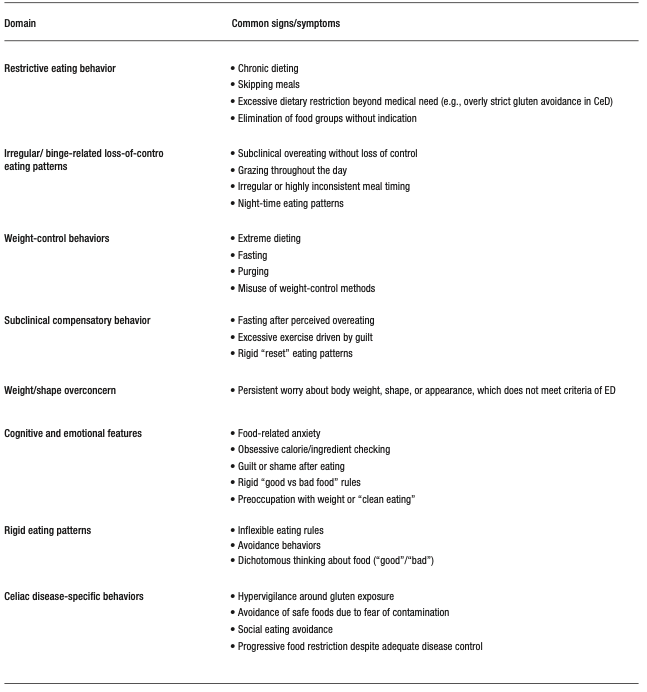
The assessment of DE in CeD requires careful distinction between adaptive adherence to a GFD and maladaptive restrictive eating behaviors that exceed medical necessity. Because DE is not a formal diagnosis but rather a broad term that encompasses problematic eating attitudes or behaviors that may be subclinical or context-specific, evaluation should include assessment of dietary rigidity, fear of gluten exposure, food-related anxiety, psychosocial impairment, nutritional status, and the impact of eating behaviors on daily functioning. Examples of DE behaviors can be found in Table 5. Tools such as the Celiac Disease Food Attitudes and Behaviors (CD-FAB) scale may help identify maladaptive food-related cognitions and behaviors, although they do not establish a psychiatric diagnosis. It is essential to consider and rule out, when appropriate, the presence of an ED, including AN, BN, BED or ARFID, since these conditions are defined psychiatric diagnosis that require specific therapeutic approaches.
Table 5. Examples of Disordered Eating Behaviors77,78
Management of Disordered Eating in Celiac Disease
Currently, there are no specific treatment guidelines for CeD that address the management of disordered eating. The available literature supports a multidisciplinary, prevention-oriented approach that integrates medical, dietary and psychological care, along with ongoing education and longitudinal monitoring.52,54,55 Where comprehensive multidisciplinary care is unavailable, a minimal pragmatic care model should include a treating physician (gastroenterologist or primary care physician) responsible for clinical evaluation and medical monitoring, a dietitian with experience in CeD to guide safe and nutritionally adequate GFD management, and referral to a mental health professional, when available, upon suspicion of underlying psychological factors or an ED, with escalation to specialized care based on clinical severity and medical risk.49,50 Given that the cornerstone of CeD management is lifelong adherence to a GFD, clinicians must carefully balance the need for strict gluten avoidance with the risk of reinforcing maladaptive eating patterns, and to prevent progression to a formal ED.56,57 In CeD, DE may arise from symptom-driven food restriction, hypervigilance defined as monitoring, worry or excessive or disproportionate avoidance behaviors related to the risk of accidental gluten ingestion or cross-contact, beyond what is reasonably required for safe disease management, or fear of adverse outcomes, all of which are amplified by the demands of strict dietary adherence.44,58 In this context, clinical follow-up should include structured and repeated assessments of eating patterns and their context, avoiding the automatic assumption that increasing restriction reflects appropriate adherence or, conversely, prematurely labeling it as psychiatric pathology.47,56
Clinical assessments should extend beyond GFD adherence to assess patterns suggestive of maladapted eating, including meal skipping, fasting to avoid symptoms, a progressive reduction in dietary variety, avoidance of safe foods, fear of eating outside the home, excessive reliance on foods prepared exclusively by the patient and persistent preoccupation with food. Additional concerning features include unintentional weight loss, body image disturbance, compensatory behaviors (e.g., purging or laxative use) and persistent gastrointestinal symptoms despite escalating restriction.56,58
There is very limited information on the routine implementation of formal screening tools for ED or DE in CeD clinics and currently there are no clinical guidelines recommending universal standardized screening for ED/DE in all CeD patients. However, selected screening instruments may support case identification in higher-risk individuals, including general ED tools such as the Eating Disorder Screen for Primary Care (ESP),59 the SCOFF questionnaire,34 as well as CeD-specific instruments such as the Celiac Disease Food Attitudes and Behaviors Scale (CD-FAB),60 which may help identify maladaptive food-related attitudes and behaviors.
Nutritional management should be carried out by dietitians with expertise in both CeD and EDs, with the goal of maintaining strict gluten exclusion while minimizing unnecessary restrictions. This includes promoting dietary variety within the GFD, clarifying the distinction between medically-required and avoidant restrictions and addressing food-related fears such as cross-contact. Psychological interventions are a core component of treatment and should target maladaptive cognition and behaviors related to food, food safety and body image. In this context, evidence-based approaches including cognitive-behavioral therapy (CBT) and family-based treatment can be adapted to address features that overlap with conditions such as ARFID and AN.
Developmental considerations are also important, as maladaptive eating behaviors often emerge during adolescence.61 In individuals with CeD, early risk factors such as dissatisfaction with body weight, symptoms of anxiety or depression, and family dynamics surrounding meals, may interact with the chronic demands of a GFD, perpetuating or exacerbating DE behaviors into adulthood.45,62 When DE behaviors are identified, clinicians should assess the patient’s medical stability and initiate early referral to mental health professionals, ideally those with expertise in EDs and familiarity with gastrointestinal conditions.56 Finally, it is essential to maintain consistent and coordinated messaging across disciplines to avoid reinforcing fear-driven eating patterns or excessive restrictions.
Nutritional Challenges in the Management of Eating Disorders and Disordered Eating in Celiac Disease
The management of EDs, particularly AN, BN and ARFID in individuals with medically prescribed restrictive diets, such as those with CeD, presents a unique therapeutic paradox. Standard EDs treatment aims to reduce rigid dietary rules, challenge food avoidance and restore flexibility in the relationship with food, whereas CeD requires strict and lifelong adherence to a gluten-free diet (GFD), creating an inherent tension between psychological recovery and medical necessity.26,63 This difficulty is especially relevant in restrictive phenotypes of EDs, in which the GFD may inadvertently reinforce restrictive cognitions or even become integrated into the disorder as a socially acceptable form of avoidance.64,65
From a nutritional perspective, maintaining a strict GFD while working to normalize eating patterns is inherently complex. A GFD requires the complete exclusion of wheat, rye, barley and related grains, as well as constant vigilance regarding hidden gluten sources and cross-contact during food processing, storage, and preparation. Without appropriate guidance, this necessary vigilance may evolve into excessive dietary restriction. Dietary management should therefore emphasize nutritionally adequate gluten-free substitutions, including whole grains and balanced meal planning to support sufficient caloric and nutrient intake.
This is particularly important given the nutritional limitations of many commercial gluten-free products, which are often not fortified with key micronutrients such as iron, folate, thiamine, riboflavin, and niacin. In a study by Jamieson et al.,66 gluten-free staple products contained 1.3 times more fat and significantly lower levels of iron (-55%), folate (-44%), and protein (-36%) compared with gluten-containing counterparts. Variability in the content and composition of fiber -particularly fermentable fiber- may contribute to the persistence of gastrointestinal symptoms and negatively affect psychological well-being in patients with CeD.67
This is exacerbated in patients with coexisting EDs, in whom insufficient intake, elimination of food groups, binge-purge behaviors and erratic eating patterns can exacerbate micronutrient deficiencies commonly seen in both conditions, such as iron, B-complex vitamins, and essential fatty acids.65,68 Altered eating behaviors may also contribute to gut microbiome dysbiosis, potentially worsening gastrointestinal symptoms and complicating dietary adherence.69 In non-restrictive ED phenotypes such as BN and BED, episodes of uncontrolled intake may increase the risk of inadvertent gluten exposure, particularly when gluten-free options are limited.64,68
DE in CeD presents overlapping but distinct nutritional challenges. Unlike formal ED, DE in CeD is often driven by symptom-related anxiety, fear of gluten exposure or excessive dietary vigilance, rather than body image concerns. Patients may progressively eliminate foods beyond what is medically necessary, reducing dietary diversity and increasing the risk of nutritional inadequacy despite the adherence to GFD.65,66 Hypervigilance around cross-contact and reliance to a GFD on a narrow repertoire of perceived “safe” foods may further impair quality of life and reinforce avoidance behaviors.63,65,70 Access to a dietitian with CeD expertise can help reduce the risk of diet stacking, whereby patients progressively adopt multiple overlapping and unnecessary dietary restrictions beyond the GFD, increasing food-related anxiety, nutritional compromise, and psychosocial burden.71
Weight changes following the onset of a GFD can further complicate management. Weight restoration in previously malnourished individuals or weight gain associated with improved absorption and increased availability of processed gluten-free foods may contribute to body image concerns, triggering DE behaviors or exacerbating pre-existing ED, particularly in adolescents and young adults.63,70 It is necessary to use standardized, evidence-based educational tools, including cross-contact checklists, which may help reduce unnecessary fear, improve consistency in counseling and support a better understanding of gluten exposure risk.72 An example of a cross-contact checklist was published in a recent review.73
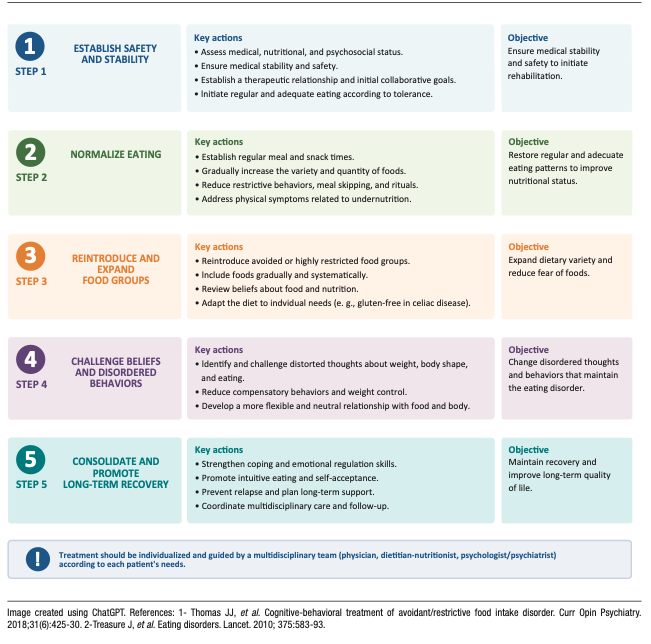
From a practical perspective, a hierarchy of nutritional goals in the management of DE begins with nutritional adequacy, prioritizing the restoration of consistent and sufficient energy intake, given that insufficient or erratic eating can worsen gastrointestinal symptoms, increase food-related anxiety and reinforce restrictive behaviors. Once adequate intake is established, the focus should shift to nutritional balance, ensuring meals that provide sufficient carbohydrates, protein and fat to promote satiety, nutritional adequacy, and more predictable digestive function. The next step is dietary variety, promoting a gradual expansion beyond a limited range of foods considered “safe”, with the goal of improving dietary diversity, nutritional quality, and confidence in eating. Only once these foundations are established should the reintroduction of specific feared or avoided foods be addressed, using a gradual and structured approach to dietary rehabilitation (Figure 2). This stepwise model aligns with established principles of nutritional rehabilitation in eating disorders , emphasizing the restoration of adequate intake, balanced nutrition, dietary variety and gradual reintroduction of feared foods.
Figure 2. Stepwise Recommendations for Dietary Rehabilitation in
Patients with Disordered Eating
Recommendations for the Clinical Management of Eating Disorders and Disordered Eating in Celiac Disease
This section provides practical guidance for clinicians managing ED and DE in individuals with CeD, with an emphasis on clinical decision-making and the delineation of roles within the care team.
In patients with restrictive eating, food-related anxiety, weight change or distress associated with the GFD, the first clinical task is to determine whether these manifestations correspond to a DE pattern or an ED requiring specialized mental health evaluation. Distinguishing between adaptive adherence to the GFD and patterns of DE or a formal ED can be challenging, as medically necessary restriction may overlap with maladaptive or pathological behaviors. Brief tools such as the SCOFF questionnaire34 or the Eating Disorder Examination Questionnaire (EDE-Q)74 support early identification in clinical settings. Severe restrictions with low weight, fear of weight gain, binge eating, compensatory behaviors or marked body image disturbance suggest an ED, whereas hypervigilance, rigid safety behaviors or progressive narrowing of food choices may reflect DE.
When an ED is suspected, the role of the physician is to recognize warning signs, assess medical stability, and facilitate a timely referral to mental health services or specialized ED programs. ED requires specialized psychiatric management; nutrition-focused interventions alone may be insufficient or they may inadvertently reinforce maladaptive behaviors. For both of these reasons, early referral is essential.
In patients with DE not meeting ED criteria, physicians and dietitians play a more active role in management. Treatment should focus on maintaining strict gluten exclusion while minimizing unnecessary dietary restriction, supporting nutritional adequacy and addressing maladaptive food-related beliefs. When patients are reluctant to engage with mental health services, clinicians should maintain longitudinal follow-up, document clinical concerns, and reconsider referral using clear, nonjudgmental language focused on functionality, safety, and quality of life.
Within this framework, several practical recommendations can guide management:
1. Assess the severity and context of altered eating behaviors to differentiate DE from ED.
2. Refer patients early when there are features consistent with an eating disorder, significant psychological distress, or nutritional risk.
3. Promote multidisciplinary collaboration with dietitians and mental health professionals experienced in both CeD and EDs.
4. Reinforce evidence-based education on GFD to prevent excessive or unnecessary restrictions.
5. Acknowledge the psychological burden of dietary vigilance, particularly in social contexts and situations of food uncertainty.
6. Conduct longitudinal monitoring of eating behaviors, nutritional status, and psychosocial impact.
Overall, management should be individualized and multidisciplinary, with a clear delineation of roles across specialties.
Figure 3 presents a summary of the diagnosis and management of EDs and DE in CeD.
Addressing Hypervigilance in Celiac Disease
Hypervigilance regarding gluten exposure warrants particular attention in the management of CeD.
While patients must develop practical skills to maintain a GFD -including reading labels, preventing cross-contact, and making safe food choices- in some individuals these behaviors may become excessively rigid or fear-driven.
In such cases, patient education is a central component of management.
Clear, evidence-based counseling from the clinical team or a dietitian specializing in CeD can help correct misconceptions about gluten exposure risk, clarify high-risk versus low-risk scenarios, and reduce uncertainty around food labeling, cross-contact, and safe practices when eating out.
The use of standardized educational tools, practical checklists, and consistent messaging among different healthcare professionals can help reduce unnecessary fears and prevent conflicting recommendations that may exacerbate anxiety.30-32
Behavioral strategies can also be helpful, particularly when hypervigilance leads to progressive restriction or psychosocial impairment.
Gradual reintroduction of unnecessarily avoided but safe foods, expansion of dietary variety and supported exposure to low-risk social eating situations can help rebuild confidence and reduce reliance on a narrow repertoire of foods perceived as “safe”.
The goal is not to reduce adherence to the GFD, but to promote proportionate vigilance which is maintaining medical safety while minimizing unnecessary restrictions, food-related anxiety and impaired quality of life.
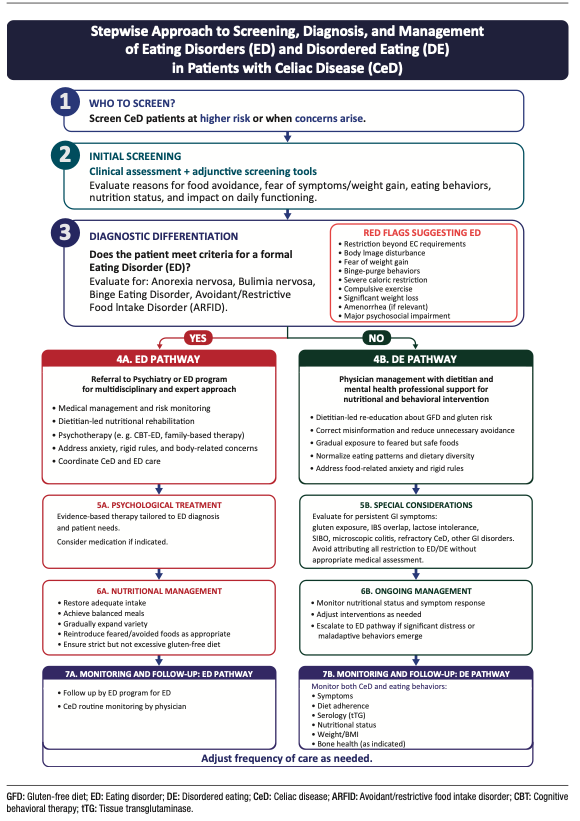
Figure 3 summarizes a stepwise approach to the screening, diagnosis, and management of eating disorders and disordered eating in celiac disease.
Figure 3. Screening, Diagnosis and Management of Eating
Disorders and Disordered Eating in Celiac Disease
The intersection between CeD, maladaptive eating behaviors and EDs represent an important and under-recognized challenge in gastroenterology. These conditions may mimic, obscure or exacerbate one another, as they share overlapping features including weight changes, abdominal pain, altered bowel habits, fatigue, micronutrient deficiencies, and malnutrition.8 (Figure 1). As a result, distinguishing between ongoing intestinal disease activity, poor dietary adherence and coexisting DE or EDs can be particularly difficult in patients with persistent symptoms or nutritional compromise despite strict dietary adherence.
This complexity is heightened by the fact that CeD treatment is inherently dietary. While strict adherence to GFD is essential, the required vigilance may contribute to hypervigilance, rigidity and food-related anxiety in susceptible individuals, potentially evolving into maladaptive eating patterns. Conversely, pre-existing EDs may interfere with treatment adherence, nutritional rehabilitation and the clinical interpretation of symptoms. These dynamics underscore the importance of distinguishing adaptive dietary management from pathological restriction as a core component of CeD care. In this context, EDs and DE should be recognized as clinically relevant factors influencing adherence, symptom persistence, nutritional risk and quality of life, justifying a multidisciplinary approach involving gastroenterologists, dietitians, and mental health professionals.
Psychosocial factors appear to play a key role in this interaction. A higher burden of symptoms consistent with EDs has been associated with depressive symptoms, lower quality of life, greater social burden, and body dissatisfaction.28,30-32 These findings support a biopsychosocial framework, although the directionality of these relationships remains unclear, as psychosocial distress may act as both a contributing factor or be a consequence of maladaptive eating behaviors. Prospective longitudinal studies are needed to clarify temporal relationships, identify predictors of progression from DE to formal ED, and determine whether targeted psychosocial interventions can improve clinical and quality-of-life outcomes in individuals with CeD.
Several important gaps in knowledge remain. First, there is limited guidance on how to adapt nutritional interventions for CeD patients with coexisting DE or ED. Standard dietary counseling, delivered in isolation, may be insufficient or may inadvertently reinforce restrictive or fear-driven behaviors. Second, there is a lack of treatment-focused evidence. Most of the available studies are cross-sectional or observational and do not evaluate the effectiveness of integrated care models. It remains unclear whether standard ED treatments require modifications in the context of CeD, or what the best strategy is for coordinating gastrointestinal, nutritional and psychiatric care.
Third, there is a lack of validated tools specifically designed to distinguish maladaptive eating behaviors from medically necessary dietary restriction. Existing instruments (e.g., EAT-26, SCOFF) were developed for the general populations and may have limited specificity in conditions requiring therapeutic dietary modification, such as CeD, food allergy, inflammatory bowel disease, eosinophilic gastrointestinal disorders or irritable bowel syndrome managed with elimination diets. Although condition-specific tools, such as the Celiac Disease Food Attitudes and Behaviors (CD-FAB) scale, show potential for identifying maladaptive food-related cognitions and behaviors in CeD, further validation and broader clinical implementation are needed.51,60
Finally, the role of social determinants of health (SDOH), including food access, health literacy and social support, remains underexplored, despite their likely influence on vulnerability to DE in CeD.
Future research should prioritize longitudinal studies that clarify the temporal relationships between CeD, DE and ED, as well as intervention trials that evaluate multidisciplinary and integrated care models. The development of assessment tools specific to CeD and the incorporation of conceptual frameworks based on the SDOH will be critical to improving both clinical care and research in this population.
Intellectual property. The authors declare that the data, figures and tables in this article are original and were carried out at their institutions.
Funding. David Armstrong is supported by the Douglas Family Chair in Nutrition Research. MIPS is supported by the Farncombe Family Digestive Health Research Institute Nutrition Initiative.
Conflict of interest. María Inés Pinto-Sanchez received research funding from Celiac Canada, Takeda and Provention Bio and an educational grant from Takeda. MIPS is member of the Scientific Medical Advisory Board of Celiac Canada.
Copyright

© 2026 Acta Gastroenterológica latinoamericana. This is an open-access article released under the terms of the Creative Commons Attribution (CC BY-NC-SA 4.0) license, which allows non-commercial use, distribution, and reproduction, provided the original author and source are acknowledged.
Cite this article as: Noejovich C V, Bhola N, Blom J J et al. Dietary Restrictions in Celiac Disease: Differential Diagnosis Between Eating Disorders and Disordered Eating Acta Gastroenterol Latinoam. 2026;56(2):154-172. https://doi.org/10.52787/agl.v56i2.653
Correspondence: María Inés Pinto-Sanchez
Email: pintosm@mcmaster.ca
Acta Gastroenterol Latinoam 2026;56(2):154-172