
Erradicación de primera línea de Helicobacter pylori con terapia dual de altas dosis versus terapia cuádruple con bismuto por 14 días: estudio multicéntrico, prospectivo y aleatorizado
DOI:
https://doi.org/10.52787/agl.v52i2.179Palabras clave:
Helicobacter pylori, terapia cuádruple con bismuto, terapia dual con dosis altas, efectos adversosResumen
Introducción. Ante la alta prevalencia de infección por Helicobacter pylori a nivel mundial y la gran resistencia de esta bacteria a los antibióticos, se ha hecho necesario el uso de terapias más agresivas para erradicar la infección. Por esta razón se propone el uso como primera línea de una terapia dual ampliada frente a la terapia cuádruple convencional utilizada para el tratamiento de esta patología.
Objetivos. Evaluar y comparar la eficacia y seguridad de la terapia cuádruple con bismuto (TCB) contra la terapia dual con dosis altas (TDA) de esomeprazol y amoxicilina como terapia empírica de primera línea para erradicar la infección por Helicobacter pylori.
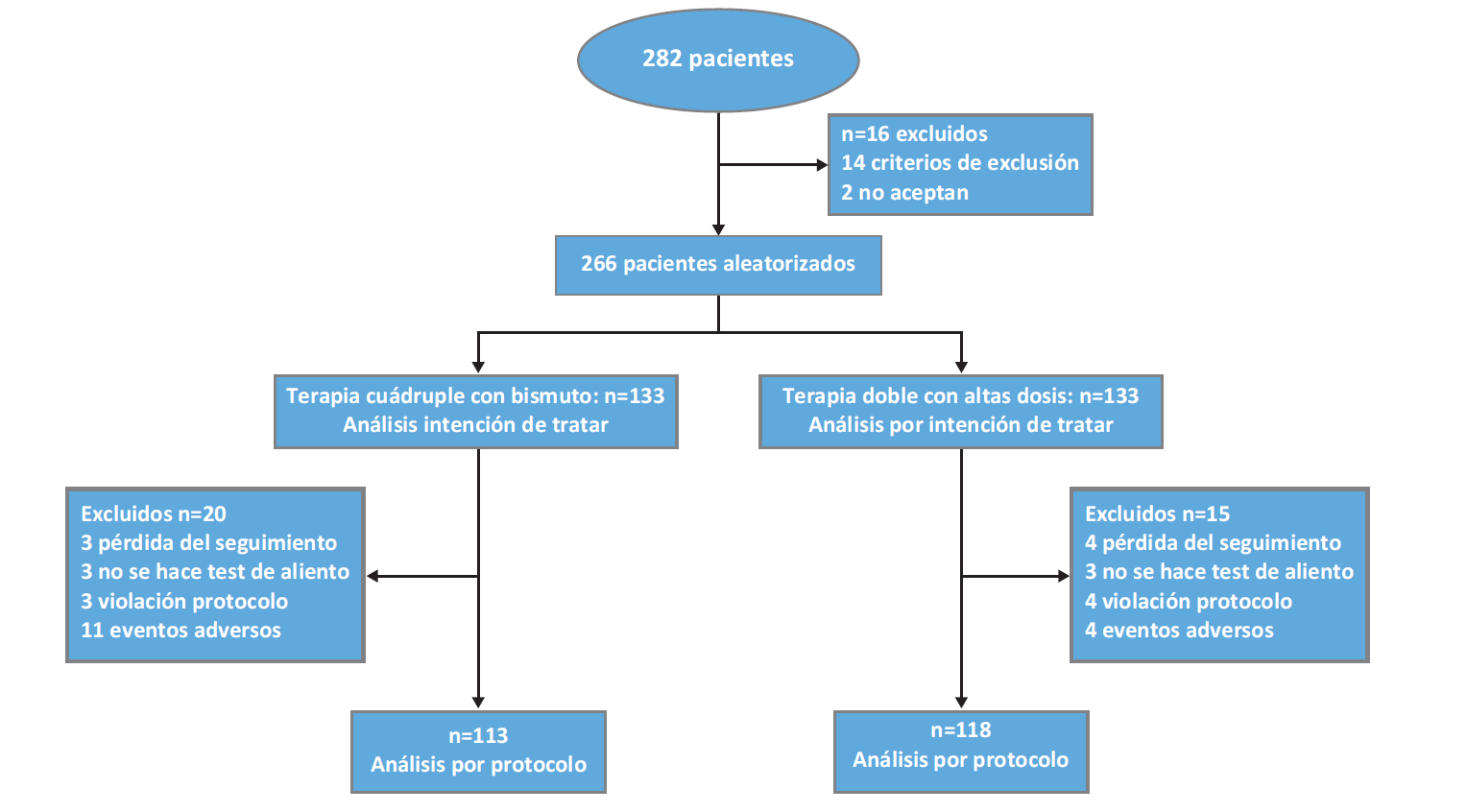
Pacientes y métodos. Ensayo prospectivo; se incluyeron 266 pacientes infectados por Helicobacter pylori sin tratamiento previo, aleatorizados para recibir terapia cuádruple con bismuto (esomeprazol 40mg dos veces por día, 2 tabletas de subsalicilato de bismuto de 262mg bid, amoxicilina 1gr bid y levofloxacina 500mg bid) por 14 días o terapia dual ampliada (esomeprazol 40mg tid, amoxicilina 1gr tid) por 14 días. La erradicación de la infección se evaluó mediante la prueba del aliento seis a ocho semanas luego de terminada la terapia. Los eventos adversos y el cumplimiento se evaluaron con cuestionarios realizados en un seguimiento telefónico o presencial.
Resultados. Las características demográficas, clínicas y endoscópicas fueron similares entre los grupos. Las tasas de erradicación por intención de tratar (133 pacientes en cada grupo) fueron del 84,9% para la TCB y del 88,7% para la TDA (p = 0,36). Las tasas de erradicación por protocolo fueron del 90.3% para la TCB y del 96,6% para la TDA (p = 0,04). La prevalencia de efectos secundarios fue del 36.8% para la TCB y del 16,5% para la TDA (p < 0,001).
Conclusiones. La terapia dual ampliada indujo una tasa de erradicación de la infección por Helicobacter pylori significativamente mayor que la terapia cuádruple con bismuto. Además, se evidencio una mayor adherencia al tratamiento con la terapia dual ampliada. Por otra parte, la terapia cuádruple con bismuto presentó mayores efectos adversos. La importancia de este estudio es la demostración de que en Colombia la terapia dual puede usarse como terapia de erradicación de primera línea para Helicobacter pylori.
Citas
-1. Jessurun J. Helicobacter pylori: an evolutionary perspective. Histopathology. 2021 Jan 1;78(1):39-47.
-2. Bravo LE, Cortes A, Carrascal E, Jaramillo R, Garcia LS, Bravo PE, et al. Helicobacter pylori: patología y prevalencia en biopsias gástricas en Colombia. Colombia Médica. 2003;34(3):124-31.
-3. Correa G. S, Cardona A. AF, Correa G. T, Correa L. LA, García G. HI, Estrada M. S. Prevalence of Helicobacter pylori and histopathological features in gastric biopsies from patients with dyspeptic symptoms at a referral center in Medellin. Revista Colombiana de Gastroenterologia. 2016 Jan 1;31(1):9-15.
-4. Roldan I, Castaño R, Navas M. Mutaciones en el gen ARNr 23S de Helicobacter pylori asociadas con resistencia a claritromicina en pacientes atendidos en una unidad de endoscopia en Medellín, Colombia. Biomédica. 2019 Aug 1;39(Supl 2):117-29.
-5. Castaño R, Ruiz M, Martínez C, Naranjo F, Campuzano-Maya G, Sanín E, et al. Evaluación para comparar dos esquemas de terapia estándar (7 frente a 10 días) contra el Helicobater pylori, con seguimiento clínico a un año. Rev Colomb Gastroenterol. 2012;27(7):80-7.
-6. Castaño R, Ruiz M, Campuzano-Maya G, Sanín F, Puerta J, Calvo-Betancur V, et al. Estudio aleatorizado comparando una primera línea de terapia estándar contra H. pylori con claritromicina versus levofloxacina por 10 días. Rev Colomb Gastroenterol. 2013;28(2):101-8.
-7. Sugano K, Tack J, Kuipers EJ, Graham DY, El-Omar EM, Miura S, et al. Kyoto global consensus report on Helicobacter pylori gastritis. Gut. 2015 Sep;64(9):1353-67.
-8. Malfertheiner P, Megraud F, ’morain O. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut. 2017;66:6-30.
-9. Bayerdörffer E, Miehlke S, Mannes GA, Sommer A, Höchter W, Weingart J, et al. Double-blind trial of omeprazole and amoxicillin to cure Helicobacter pylori infection in patients with duodenal ulcers. Gastroenterology. 1995;108(5):1412-7.
-10. Miehlke S, Mannes GA, Lehn N, Hele C, Stolte M, Bayerdörffer E. An increasing dose of omeprazole combined with amoxycillin cures Helicobacter pylori infection more effectively. Alimentary Pharmacology and Therapeutics. 1997;11(2):323-9.
-11. Zullo A, Ridola L, De Francesco V, Gatta L, Hassan C, Alvaro D, et al. High-dose esomeprazole and amoxicillin dual therapy for first-line Helicobacter pylori eradication: A proof of concept study. Annals of Gastroenterology. 2015;28(4):448-51.
-12. Sapmaz F, Kalkan IH, Atasoy P, Basyigit S, Guliter S. A Non-Inferiority Study : Modified Dual Therapy Consisting Higher Doses of Rabeprazole Is as Successful as Standard Quadruple Therapy in Eradication of Helicobacter pylori. 2015;6:1-6.
-13. Yang JC, Lin CJ, Wang HL, Chen J De, Kao JY, Shun CT, et al. High-dose dual therapy is superior to standard first-line or rescue therapy for Helicobacter pylori infection. Clinical Gastroenterology and Hepatology. 2015;13(5):895-905.e5.
-14. Zhu YJ, Zhang Y, Wang TY, Zhao JT, Zhao Z, Zhu JR, et al. High dose PPI-amoxicillin dual therapy for the treatment of Helicobacter pylori infection: a systematic review with meta-analysis. Therapeutic Advances in Gastroenterology. 2020;13:1-12.
-15. Yang X, Wang JX, Han SX, Gao CP. High dose dual therapy versus bismuth quadruple therapy for Helicobacter pylori eradication treatment: A systematic review and meta-analysis. Medicine (United States). 2019;98(7):1-7.
-16. Shah SC, Iyer PG, Moss SF. AGA Clinical Practice Update on the Management of Refractory Helicobacter pylori Infection: Expert Review. Gastroenterology. 2021 Apr 1;160(5):1831-41.
-17. Zagari RM, Frazzoni L, Marasco G, Fuccio L, BAZZOLi F. Treatment of Helicobacter pylori infection: A clinical practice update. Vol. 112, Minerva Medica. Edizioni Minerva Medica; 2021. p. 281-7.
-18. Zullo A. The current role of dual therapy for treatment of Helicobacter pylori: Back to the future? European Journal of Gastroenterology and Hepatology. 2020;32(5):555-6.
-19. Shah SC, Iyer PG, Moss SF. AGA Clinical Practice Update on the Management of Refractory Helicobacter pylori Infection: Expert Review. Gastroenterology. 2021;160(5):1831-41.
-20. Caldas M, Pérez-Aisa Á, Castro-Fernández M, Bujanda L, Lucendo AJ, Rodrigo L, et al. European registry on Helicobacter pylori management: Effectiveness of first and second-line treatment in Spain. Antibiotics. 2021;10(1):1-15.
-21. Megraud F, Bruyndonckx R, Coenen S, Wittkop L, Huang TD, Hoebeke M, et al. Helicobacter pylori resistance to antibiotics in Europe in 2018 and its relationship to antibiotic consumption in the community. Gut. 2021 May 10.
-22. Yun J, Wu Z, Qi G, Han T, Zhang D. The high-dose amoxicillin-proton pump inhibitor dual therapy in eradication of Helicobacter pylori infection. Expert Review of Gastroenterology and Hepatology. 2021;15(2):149-57.
-23. Buitrago-Laguado EJ, Ruiz-Linares CE. Tesis - Eficacia de la terapia dual para erradicación de H. pylori en una población colombiana. [Bogotá]: Universidad Nacional de Colombia; 2021.
-24. Lima JJ, Thomas CD, Barbarino J, Desta Z, Van Driest SL, El Rouby N, et al. Clinical Pharmacogenetics Implementation Consortium (CPIC) Guideline for CYP2C19 and Proton Pump Inhibitor Dosing. Clinical Pharmacology and Therapeutics. 2020;0(0):1-7.
-25. Arévalo-Galvis A, Otero-Regino WA, Ovalle-Celis GN, Rodríguez-Gómez ER, Trespalacios-Rangel AA. Prevalence of CYP2C19 polymorphism in Bogotá, Colombia: The first report of allele *17. PLoS ONE. 2021;16(1 January 2021):1-12.
-26. Díaz-Ordóñez L, Ramírez-Montaño D, Candelo E, González-Restrepo C, Silva-Peña S, Rojas CA, et al. Evaluation of CYP2C19 Gene Polymorphisms in Patients with Acid Peptic Disorders Treated with Esomeprazole. Pharmacogenomics and Personalized Medicine. 2021 Apr;Volume 14:509-20.
-27. Sahara S, Sugimoto M, Uotani T, Ichikawa H, Yamade M, Kagami T, et al. Potent gastric acid inhibition over 24 hours by 4-times daily dosing of esomeprazole 20 mg. Digestion. 2015 Jun 15;91(4):277-85.
-28. Wang YC, Chen YP, Ho CY, Liu TW, Chu CH, Wang HY, et al. The Impact of Gastric Juice pH on the Intraluminal Therapy for Helicobacter pylori Infection. J Clin Med. 2020 Jun 14;9(6):1852.
-29. Zhu YJ, Zhang Y, Wang TY, Zhao JT, Zhao Z, Zhu JR, et al. High dose PPI-amoxicillin dual therapy for the treatment of Helicobacter pylori infection: a systematic review with meta-analysis. Vol. 13, Therapeutic Advances in Gastroenterology. SAGE Publications Ltd; 2020.
-30. Yu L, Luo L, Long X, Liang X, Ji Y, Graham DY, et al. High-dose PPI-amoxicillin dual therapy with or without bismuth for first-line Helicobacter pylori therapy: A randomized trial. Helicobacter. 2019 Aug 1;24(4).
-31. Trespalacios-Rangél AA, Otero W, Arévalo-Galvis A, Poutou-Piñales RA, Rimbara E, Graham DY. Surveillance of levofloxacin resistance in helicobacter pylori isolates in Bogotá-Colombia (2009-2014). PLoS ONE. 2016 Jul 1;11(7).
-32. Miehlke S, Hansky K, Schneider-Brachert W, Kirsch C, Morgner A, Madisch A, et al. Randomized trial of rifabutin-based triple therapy and high-dose dual therapy for rescue treatment of Helicobacter pylori resistant to both metronidazole and clarithromycin. Alimentary Pharmacology and Therapeutics. 2006 Jul;24(2):395-403.
-33. Furuta T, Shirai N, Kodaira M, Sugimoto M, Nogaki A, Kuriyama S, et al. Pharmacogenomics-based tailored versus standard therapeutic regimen for eradication of H. pylori. Clinical Pharmacology and Therapeutics. 2007 May 10;81(4):521-8.
-34. Graham DY, Javed SU, Keihanian S, Abudayyeh S, Opekun AR. Dual proton pump inhibitor plus amoxicillin as an empiric anti-H. pylori therapy: Studies from the United States. Journal of Gastroenterology. 2010;45(8):816-20.
-35. Ince AT, Tozlu M, Baysal B, Şentürk H, Arici S, Oz̈den A. Yields of dual therapy containing high-dose proton pump inhibitor in eradication of H. pylori positive dyspeptic patients. Hepato-Gastroenterology. 2014 Jul 1;61(133):1454-8.
-36. Attumi TA, Graham DY. High-Dose Extended-Release Lansoprazole (Dexlansoprazole) and Amoxicillin Dual Therapy for Helicobacter pylori Infections. Helicobacter. 2014;19(4):319-22.
-37. Kwack W, Lim Y, Lim C, Graham DY. High Dose Ilaprazole/Amoxicillin as First-Line Regimen for Helicobacter pylori Infection in Korea. Gastroenterol Res Pract. 2016;2016:1648047.
-38. Zhou C, Hu Y, Xiao Y, Yin W. Current treatment of tracheoesophageal fistula. Ther Adv Respir Dis. 2017;11(4):173-80.
-39. Tai WC, Liang CM, Kuo CM, Huang PY, Wu CK, Yang SC, et al. A 14 day esomeprazole- And amoxicillin-containing high-dose dual therapy regimen achieves a high eradication rate as first-line anti-Helicobacter pylori treatment in Taiwan: a prospective randomized trial. Journal of Antimicrobial Chemotherapy. 2019;74(6):1718-24.
-40. Yu L, Luo L, Long X, Liang X, Ji Y, Graham DY, et al. High-dose PPI-amoxicillin dual therapy with or without bismuth for first-line Helicobacter pylori therapy: A randomized trial. Helicobacter. 2019 Aug 1;24(4).
-41. Yang J, Zhang Y, Fan L, Zhu YJ, Wang TY, Wang XW, et al. Eradication Efficacy of Modified Dual Therapy Compared with Bismuth-Containing Quadruple Therapy as a First-Line Treatment of Helicobacter pylori. American Journal of Gastroenterology. 2019;114(3):437-45.
-42. Öztürk K, Kurt Ö, Çelebi G, Şarlak H, Karakaya MF, Demirci H, et al. High-dose dual therapy is effective as first-line treatment for Helicobacter pylori infection. Turkish Journal of Gastroenterology. 2020;31(3):234-8.
-43. Meriem Z, Elmekkaoui A, Bouqfar M, Zazour A, Khannoussi W, Kharrasse G, et al. Non-Bismuth Quadruple Therapy, Sequential Therapy or High-Dose Esomeprazole and Amoxicillin Dual Therapy for First-Line Helicobacter pylori Eradication: A Prospective Randomized Study. Cureus. 2020;12(12).
-44. Hwong-Ruey Leow A, Chang JV, Goh KL. Searching for an optimal therapy for H. pylori eradication: High-dose proton-pump inhibitor dual therapy with amoxicillin vs. standard triple therapy for 14 days. Helicobacter. 2020;25(5):10-4.
-45. Abadi ATB, Ierardi E. Vonoprazan and Helicobacter pylori treatment: A lesson from Japan or a limited geographic phenomenon? Vol. 10, Frontiers in Pharmacology. Frontiers Media S.A.; 2019.
-46. Furuta T, Yamade M, Kagami T, Uotani T, Suzuki T, Higuchi T, et al. Dual Therapy with Vonoprazan and Amoxicillin Is as Effective as Triple Therapy with Vonoprazan, Amoxicillin and Clarithromycin for Eradication of Helicobacter pylori. Vol. 101, Digestion. S. Karger AG; 2020. p. 743–51.
Publicado
Cómo citar
Número
Sección
Licencia
Derechos de autor 2022 Rodrigo Castaño Llano, Amy Piñeres, Jeronimo Toro Calle, Sandra Molina Meneses, William Valencia Gomez, Juan Esteban Puerta Botero

Esta obra está bajo una licencia internacional Creative Commons Atribución-NoComercial-CompartirIgual 4.0.









