
Efficacy and Safety of Endoscopic Clousure of Gastrointestinal Fistulas Using a New Endoscopic Suturing System (X-Tack) in Colombia: A Case Series
DOI:
https://doi.org/10.52787/agl.v56i2.627Keywords:
Gastrointestinal fistula, endoscopic closure, endoscopic suturing, X-Tack™, therapeutic endoscopyAbstract
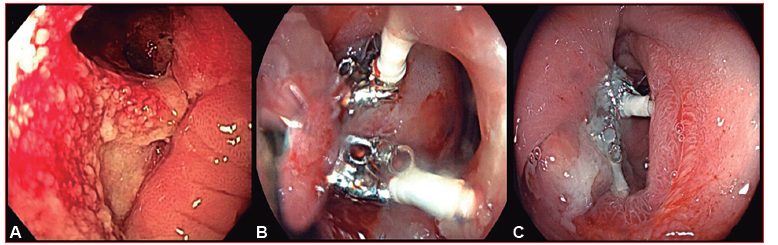
Introduction. Gastrointestinal fistulas are uncommon but potentially severe conditions associated with infectious collections, bleeding, sepsis, malnutrition, and increased morbidity and mortality. Advances in therapeutic endoscopy have expanded the options for minimally invasive treatment. Endoscopic therapy has become a first-line treatment strategy for colorectal anastomotic leaks and fistulas. In esophageal and gastric fistulas, esophageal stents remain a widely used alternative, although their tolerability may be limited by the location of the defect. The X-Tack™ endoscopic suturing system (Boston Scientific), introduced in 2020, enables closure of anatomical defects through the working channel of the endoscope without requiring scope withdrawal, facilitating access to complex anatomical locations and larger defects.
Patients and Methods. We present a case series of nine gastrointestinal fistula defects in eight patients treated in Colombia. The defects were located in the proximal esophagus, stomach, duodenum, colon, and rectum. In all cases, the X-Tack™ endoscopic suturing system was used as part of the therapeutic strategy for defect management.
Results. The mean patient age was 56.5 years, and 62.5% were male. The esophagus was the most frequent location (50%). The predominant suture pattern was the “Z” configuration (87.5%). Endoscopic closure of the anatomical defect was successfully achieved in all cases, with no procedure-related adverse events and complete clinical resolution during the reported follow-up period.
Conclusions. In this case series, the X-Tack™ system was used as part of a multimodal therapeutic strategy for the management of complex gastrointestinal fistulas at different anatomical locations. Its use enabled successful closure of all treated defects without procedure-related complications and with clinical resolution, suggesting that it may represent a feasible and safe therapeutic option in selected patients. Prospective studies including larger numbers of patients are needed to better define its role within the therapeutic algorithm for gastrointestinal fistulas.
References
-1. Gonzalez-Pinto I, Gonzalez EM. Optimising the treatment of upper gastrointestinal fistulae. Gut. 2001;49(Suppl 4). DOI: 10.1136/gut.49.suppl_4.21
-2. Almasaid S, Suhail FK, Khan HM. Endoscopic through-the-scope X-Tack helix suturing system for complete closure of a large full-thickness after surgical gastric perforation. ACG Case Rep J. 2024;11(9):e01493. DOI:10.14309/crj.0000000000001493
-3. Bemelman WA, Baron TH. Endoscopic management of transmural defects, including leaks, perforations, and fistulae. Gastroenterology. 2018. DOI:10.1053/j.gastro.2018.01.067
-4. Zhang LY, Bejjani M, Ghandour B, Khashab MA. Endoscopic through-the-scope suturing. VideoGIE. 2022;7(1):1-3. DOI:10.1016/j.vgie.2021.08.006
-5. Canakis A, Dawod SM, Dawod, et al. Efficacy, feasibility, and safety of the X-Tack endoscopic HeliX tacking system: A multicenter experience. J Clin Gastroenterol. 2024;58(10):1052-1057. DOI:10.1097/MCG.0000000000001977
-6. Awadalla M, Trasolini R, Stones J, Berzin T. The X-Tack endoscopic helix tacking system: a single tertiary center experience [abstract]. Am J Gastroenterol. 2023; ACG Annual Scientific Meeting.
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 Javier Alberto Preciado Aponte, Elkin Julián Suárez Angarita, Alejandro Concha Mejía, Manuel Alonso Ardila Báez

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









