
Unmasking the Burden of Cannabis in Cirrhosis: A Propensity-Matched Real-World Analysis
DOI:
https://doi.org/10.52787/agl.v56i2.592Keywords:
Cannabis use disorder, cirrhosis, electrolyte derangement, pneumonia, ICU admissionAbstract
Introduction. Cannabis use is increasingly prevalent among patients with liver disease, but its clinical impact on outcomes in cirrhosis remains unclear. This study evaluated the association between cannabis use disorder and clinical complications in patients with cirrhosis.
Methods. We conducted a retrospective study using the TriNetX network. Adults aged 18–89 years with cirrhosis were divided into two cohorts: those with cannabis use disorder (n = 46,347) and those without (n = 888,138). Propensity score matching (1:1) was performed using demographic characteristics and key laboratory values. The final matched sample consisted of 46,168 patients in each group. Outcomes were assessed over a 1-year follow-up and included all-cause mortality, critical care admission, respiratory complications, dyselectrolytemia, and hypoalbuminemia.
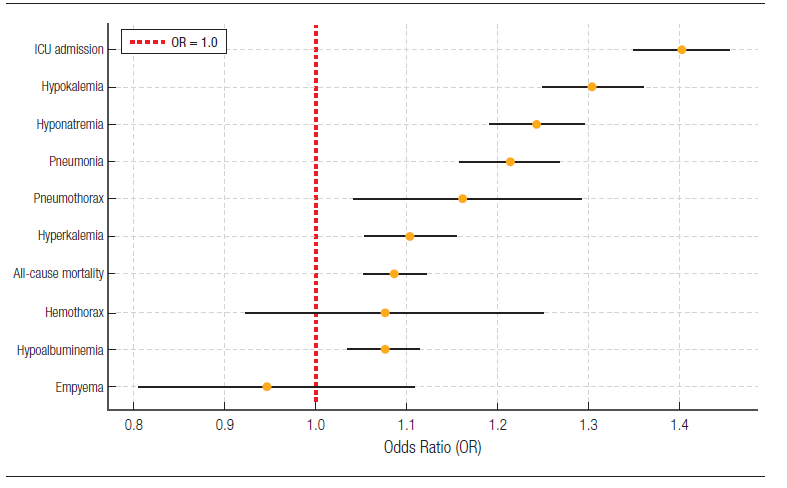
Results. Patients with cannabis use disorder had significantly higher odds of all-cause mortality (OR 1.086, 95% CI 1.052–1.121), critical care admission (OR 1.400, 95% CI 1.348–1.453), pneumonia (OR 1.212, 95% CI 1.158–1.268), pneumothorax (OR 1.160, 95% CI 1.041–1.293), and hypoalbuminemia (OR 1.074, 95% CI 1.035–1.114). Hyponatremia (OR 1.241, 95% CI 1.191–1.293), hyperkalemia (OR 1.102, 95% CI 1.053–1.154), and hypokalemia (OR 1.302, 95% CI 1.248–1.359) were also more frequent in the cannabis group. No significant associations were observed for hemothorax (OR 1.074, 95% CI 0.922–1.251) or empyema (OR 0.945, 95% CI 0.805–1.109).
Conclusion. These observational findings suggest that documented cannabis use disorder may identify a higher-risk subgroup among patients with cirrhosis, although they do not establish causality. Clinicians may consider evaluating cannabis use as part of risk assessment and patient counseling. Further prospective studies are needed to better define the mechanisms and long-term impact of cannabis use in advanced liver disease.
References
-1. Sharma B, John S. Hepatic Cirrhosis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [cited 2025 Oct 13]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK482419/
-2. FastStats [Internet]. 2025 [cited 2025 Oct 14]. Available from: https://www.cdc.gov/nchs/fastats/liver-disease.htm
-3. Tapper EB, Parikh ND. Mortality due to cirrhosis and liver cancer in the United States, 1999-2016: observational study. BMJ. 2018;362:k2817.
-4. Scaglione S, Kliethermes S, Cao G, Shoham D, Durazo R, Luke A, et al. The epidemiology of cirrhosis in the United States: a population-based study. J Clin Gastroenterol. 2015;49(8):690-696.
-5. Serper M, Tapper EB, Kaplan DE, Taddei TH, Mahmud N. Patterns of care utilization and hepatocellular carcinoma surveillance: tracking care across the pandemic. Am J Gastroenterol. 2023;118(2):294-303.
-6. Rubin JB, Loeb R, Shen H, Hoggatt K, Keyhani S, Lai J. Trends and predictors of cannabis use among 410,215 veterans with cirrhosis, 2010-2021. Am J Gastroenterol. 2024;119(10 Suppl):S1312.
-7. Azofeifa A. National estimates of marijuana use and related indicators - National Survey on Drug Use and Health, United States, 2002-2014. MMWR Surveill Summ [Internet]. 2016 [cited 2025 Oct 14]. Available from: https://www.cdc.gov/mmwr/volumes/65/ss/ss6511a1.htm
-8. Wang Y, Mukhopadhyay P, Cao Z, Wang H, Feng D, Haskó G, et al. Cannabidiol attenuates alcohol-induced liver steatosis, metabolic dysregulation, inflammation and neutrophil-mediated injury. Sci Rep. 2017;7(1):12064.
-9. Siegmund SV, Schwabe RF. Endocannabinoids and liver disease. II. Endocannabinoids in the pathogenesis and treatment of liver fibrosis. Am J Physiol Gastrointest Liver Physiol. 2008;294(2):G357-G362.
-10. Adejumo AC, Alliu S, Ajayi TO, Adejumo KL, Adegbala OM, Onyeakusi NE, et al. Cannabis use is associated with reduced prevalence of non-alcoholic fatty liver disease: a cross-sectional study. PLoS One. 2017;12(4):e0176416.
-11. Adejumo AC, Ajayi TO, Adegbala OM, Adejumo KL, Alliu S, Akinjero AM, et al. Cannabis use is associated with reduced prevalence of progressive stages of alcoholic liver disease. Liver Int. 2018;38(8):1475-1486.
-12. Choi CJ, Weiss SH, Nasir UM, Pyrsopoulos NT. Cannabis use history is associated with increased prevalence of ascites among patients with nonalcoholic fatty liver disease: a nationwide analysis. World J Hepatol. 2020;12(11):993-1003.
-13. TriNetX [Internet]. [cited 2025 Oct 14]. Real-world data for the life sciences and healthcare. Available from: https://trinetx.com/
-14. Bhaskar A, Bell A, Boivin M, Briques W, Brown M, Clarke H, et al. Consensus recommendations on dosing and administration of medical cannabis to treat chronic pain: results of a modified Delphi process. J Cannabis Res. 2021;3(1):22.
-15. Mallat A, Teixeira-Clerc F, Deveaux V, Manin S, Lotersztajn S. The endocannabinoid system as a key mediator during liver diseases: new insights and therapeutic openings. Br J Pharmacol. 2011;163(7):1432-1440.
-16. Julien B, Grenard P, Teixeira-Clerc F, Van Nhieu JT, Li L, Karsak M, et al. Antifibrogenic role of the cannabinoid receptor CB2 in the liver. Gastroenterology. 2005;128(3):742-755.
-17. Silvestri C, Paris D, Martella A, Melck D, Guadagnino I, Cawthorne M, et al. Two non-psychoactive cannabinoids reduce intracellular lipid levels and inhibit hepatosteatosis. J Hepatol. 2015;62(6):1382-1390.
-18. Patsenker E, Stickel F. Cannabinoids in liver diseases. Clin Liver Dis. 2016;7(2):21-25.
-19. Jadoon KA, Ratcliffe SH, Barrett DA, Thomas EL, Stott C, Bell JD, et al. Efficacy and safety of cannabidiol and tetrahydrocannabivarin on glycemic and lipid parameters in patients with type 2 diabetes: a randomized, double-blind, placebo-controlled, parallel-group pilot study. Diabetes Care. 2016;39(10):1777-1786.
-20. Cohen-Naftaly M, Friedman SL. Current status of novel antifibrotic therapies in patients with chronic liver disease. Ther Adv Gastroenterol. 2011;4(6):391-417.
-21. Iredale JP. Models of liver fibrosis: exploring the dynamic nature of inflammation and repair in a solid organ. J Clin Invest. 2007;117(3):539-548.
-22. Puche JE, Saiman Y, Friedman SL. Hepatic stellate cells and liver fibrosis. Compr Physiol. 2013;3(4):1473-1492.
-23. Hernandez-Gea V, Friedman SL. Pathogenesis of liver fibrosis. Annu Rev Pathol. 2011;6:425-456.
-24. Mattingly DT, Richardson MK, Hart JL. Prevalence of and trends in current cannabis use among US youth and adults, 2013-2022. Drug Alcohol Depend Rep. 2024;12:100253.
-25. Sobotka LA, Mumtaz K, Hinton A, Kelly SG, Conteh LF, Michaels AJ, et al. Cannabis use may reduce healthcare utilization and improve hospital outcomes in patients with cirrhosis. Ann Hepatol. 2021;23:100280.
-26. Zhao E, Kabaria S, Patel AV. Cannabis use decreases morbidity and mortality among cirrhosis patients: a national cohort study. Am J Gastroenterol. 2021;116:S569.
-27. Wijarnpreecha K, Panjawatanan P, Ungprasert P. Use of cannabis and risk of advanced liver fibrosis in patients with chronic hepatitis C virus infection: a systematic review and meta-analysis. J Evid Based Med. 2018;11(4):272-277.
-28. Vozoris NT, Zhu J, Ryan CM, Chow CW, To T. Cannabis use and risks of respiratory and all-cause morbidity and mortality: a population-based, data-linkage cohort study. BMJ Open Respir Res. 2022;9(1):e001216.
-29. Renger L, Dhanani J, Milford E, Tabah A, Shekar K, Ramanan M, et al. Cannabis use disorders and outcome of admission to intensive care: a retrospective multicentre cohort study. J Crit Care. 2024;80:154504.
-30. Tashkin DP. Marijuana and lung disease. Chest. 2018;154(3):653-663.
-31. Bisconti M, Marulli G, Pacifici R, Sollitto F, Nex G, Trabucco X, et al. Cannabinoids identification in lung tissues of young cannabis smokers operated for primary spontaneous pneumothorax and correlation with pathologic findings. Respiration. 2019;98(6):503-511.
-32. Hedevang Olesen W, Katballe N, Sindby JE, Titlestad IL, Andersen PE, Ekholm O, et al. Cannabis increased the risk of primary spontaneous pneumothorax in tobacco smokers: a case-control study. Eur J Cardiothorac Surg. 2017;52(4):679-685.
-33. Aujayeb A, Donald C, Doe S. Breath-holding in a marijuana smoker. Respir Med Case Rep. 2012;5:69-72.
-34. Gulhar R, Ashraf MA, Jialal I. Physiology, acute phase reactants. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [cited 2025 Oct 18]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK519570/
-35. Lai JC, Tandon P, Bernal W, Tapper EB, Ekong U, Dasarathy S, et al. Malnutrition, frailty, and sarcopenia in patients with cirrhosis: 2021 practice guidance by the American Association for the Study of Liver Diseases. Hepatology. 2021;74(3):1611-1644.
-36. Allen JH, de Moore GM, Heddle R, Twartz JC. Cannabinoid hyperemesis: cyclical hyperemesis in association with chronic cannabis abuse. Gut. 2004;53(11):1566-1570.
-37. Simonetto DA, Oxentenko AS, Herman ML, Szostek JH. Cannabinoid hyperemesis: a case series of 98 patients. Mayo Clin Proc. 2012;87(2):114-119.
-38. Habboushe J, Sedor J. Cannabinoid hyperemesis acute renal failure: a common sequela of cannabinoid hyperemesis syndrome. Am J Emerg Med. 2014;32(6):690.e1-690.e2.
-39. Abodunde OA, Nakda J, Nweke N, Veera RL. Cannabinoid hyperemesis syndrome presenting with recurrent acute renal failure. J Med Cases. 2013;4(3):173-175.
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 FNU Alvina, Chidera N Onwuzo, Azhar Hussain, Adaora Ojiugo Moka, Rashid Abdel Razeq, Somtochukwu Onwuzo

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









