
Redefining the Initial Endoscopy Evaluation of Esophageal Symptoms: Toward a PrecisionBased Diagnostic Paradigm
DOI:
https://doi.org/10.52787/agl.v56i1.601Abstract
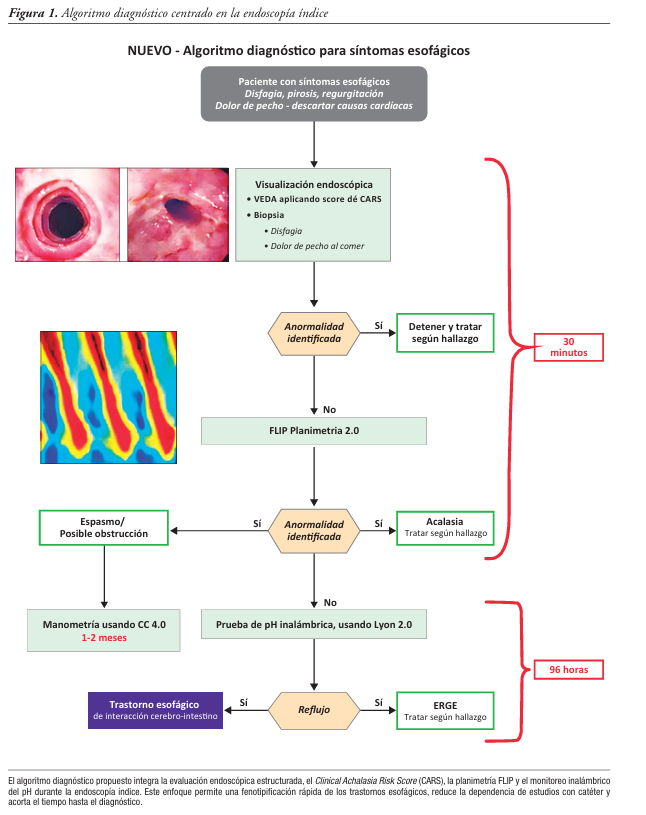
Esophageal symptoms -including dysphagia, heartburn, regurgitation, and non-cardiogenic chest pain- are among the most common indications for referral to gastroenterology. Despite their high prevalence, establishing a definitive etiological diagnosis remains a significant clinical challenge due to the marked overlap in symptom profiles between gastroesophageal reflux disease, eosinophilic esophagitis, esophageal motility disorders, and disorders of gut–brain interaction. Current diagnostic paradigms are generally based on sequential testing strategies that often begin with empirical treatment with proton pump inhibitor followed by endoscopy and, when this is inconclusive, catheter-based esophageal functional studies. This approach is associated with prolonged diagnostic times, incomplete studies due to poor tolerance, delays in access to specialized centers, and substantial increase in healthcare costs. Recent advances in endoscopic and physiologic technologies offer the opportunity to fundamentally reframe the evaluation of esophageal symptoms. The integration of endoscopic risk stratification tools, such as the Clinical Achalasia Risk Score, Functional Lumen Imaging Probe panometry, and wireless pH monitoring, enables a comprehensive physiologic evaluation during the index endoscopy under sedation, optimizing the diagnostic performance of the procedure. This strategy has the potential to significantly reduce diagnostic uncertainty, shorten the time to definitive diagnosis, and decrease reliance on poorly tolerated catheter studies. This review synthesizes the emerging evidence supporting a diagnostic paradigm centered on index endoscopy as a central and integrative diagnostic event. The limitations of traditional diagnostic methods are analyzed and the physiological principles and clinical utility of planimetry using Functional Lumen Imaging Probe and wireless reflux monitoring are reviewed. A practical algorithm integrating these tools is proposed, with the aim of providing accurate and efficient care, aimed at improving diagnostic performance and therapeutic decision-making in patients with esophageal symptoms. Given that the available evidence is still emerging and concentrated in centers with experience, the proposed algorithm should be interpreted as a pragmatic framework for optimizing the diagnostic sequence, subject to prospective validation and adaptation to the local context.
References
-1. Aziz Q, Fass R, Gyawali CP, Miwa H, Pandolfino JE, Zerbib F. Functional esophageal disorders. Gastroenterology. 2016;150(6):1368-1379. DOI: 10.1053/j.gastro.2016.02.012
-2. Veldhuyzen van Zanten SJ, et al. Diagnostic delay in refractory GERD. Am J Gastroenterol. 2006;101(11):2457-2462.
-3. Kessing BF, et al. Esophageal achalasia: diagnostic delay and clinical impact. Dis Esophagus. 2014;27(7):641-648.
-4. Ellison A, Peller M, Nguyen AD, Carlson DA, Pandolfino JE, Triggs JR, et al. An endoscopic scoring system for achalasia: the CARS score. Gastrointest Endosc. 2024;100(3):417-428.e1.
-5. Carlson DA, Li M, Fass O, Pitisuttithum P, Goudie E, Kou W, et al. A combined endoscopy and functional lumen imaging probe planimetry approach can expedite diagnosis of esophageal motility disorders. Gastrointest Endosc. 2025;102(6):811-821.e4. DOI: 10.1016/j.gie.2025.03.1329
-6. Gyawali CP, et al. Evaluation of GERD symptoms beyond PPI response. Clin Gastroenterol Hepatol. 2018;16(7):984-990.
-7. Taft TH, Carlson DA, Marchese SH, Triggs JR, Pandolfino JE. Initial assessment of medical post-traumatic stress among patients with chronic esophageal diseases. Neurogastroenterol Motil. 2023;35(5):e14540.
-8. Lundell LR, Dent J, Bennett JR, Blum AL, Armstrong D, Galmiche JP, et al. Endoscopic assessment of oesophagitis: clinical and functional correlates. Gut. 1999;45(2):172-180.
-9. Carlson DA, Gyawali CP, Khan A, Huo D, Pandolfino JE. Classifying esophageal motility by FLIP planimetry. Am J Gastroenterol. 2021;116(12):2357-2366.
-10. Carlson DA, Prescott JE, Baumann AJ, Kou W, Pandolfino JE. Validation of secondary peristalsis classification using FLIP planimetry. Neurogastroenterol Motil. 2021;33(11):e14192.
-11. Carlson DA, Baumann AJ, Prescott JE, Hungness ES, Pandolfino JE. Validation of clinically relevant thresholds of EGJ obstruction using FLIP planimetry. Clin Gastroenterol Hepatol. 2022;20(6):e1250-e1262.
-12. Carlson DA, Baumann AJ, Prescott JE, Triggs JR, Kou W, Kahrilas PJ, et al. A standardized approach to performing and interpreting functional lumen imaging probe planimetry for esophageal motility disorders: the Dallas Consensus. Gastroenterology. 2025;168(6):1114-1127.e5. DOI: 10.1053/j.gastro.2025.01.234
-13. Pandolfino JE, et al. Wireless pH monitoring: clinical utility. Am J Gastroenterol. 2003;98(4):740-749.
-14. Yadlapati R, Pandolfino JE, Fox MR, Gyawali CP, Roman S. Lyon Consensus 2.0. Gastroenterology. 2023;164(5):e1-e35.
-15. Shah SC, et al. Cost-effectiveness of physiologic testing in heartburn. Gastroenterology. 2022;163(1):44-57.
-16. Shah SC, et al. Cost-effectiveness of early motility testing in dysphagia. Clin Gastroenterol Hepatol. 2023;21(4):921-930.
-17. Hashimoto H, et al. Prolonged wireless pH monitoring increases diagnostic yield in patients with reflux symptoms and borderline 24-hour impedance pH. Dis Esophagus. 2025;38(2):doaf030. DOI: 10.1093/dote/doaf030
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 Juan I Olmos, John E Pandolfino

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









