
Re-Engagement of Hepatitis C Patients Lost to Follow-Up: A Multicenter Study from Argentina
DOI:
https://doi.org/10.52787/agl.v56i2.604Keywords:
Hepatitis C, patient dropouts, health services accessibility, treatment outcome, ArgentinaAbstract
Background and aims. Many anti-HCV-positive individuals in Argentina remain lost to follow-up. We assessed a multicenter re-engagement program using complementary case-finding strategies, described the care cascade, and evaluated treatment outcomes.
Methods. Five public hospitals implemented two strategies: laboratory-based screening at a tertiary hospital and its primary/secondary network, and combined medical record/laboratory searches at four tertiary hospitals to identify prior anti-HCV-positive individuals. Lost to follow-up was operationally defined as no documented hepatology care, HCV RNA testing, or antiviral treatment within participating institutions for ≥ 12 months. A two-visit pathway was offered. Primary outcomes were re-engagement, treatment initiation, and sustained virologic response at 12 weeks (SVR12); secondary outcomes were fibrosis stage and SVR4-SVR12 concordance. As an exploratory objective, all-cause mortality was assessed in the laboratory cohort using conditional logistic regression.
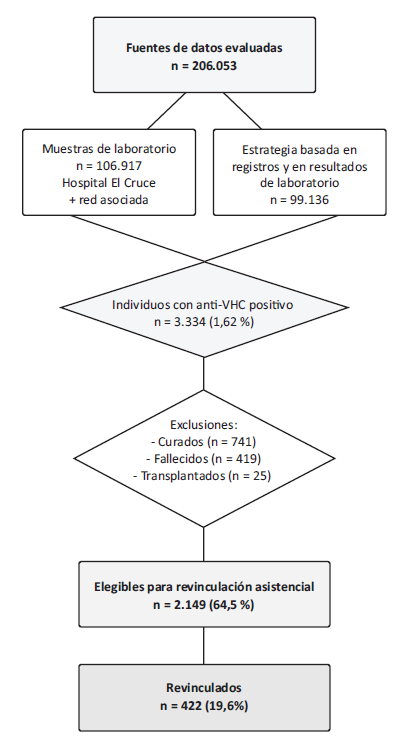
Results. Across 206,053 data sources (106,917 laboratory samples and 99,136 medical records), 3,334 individuals were anti-HCV positive. After excluding patients who had been cured (n = 741), were deceased (n = 419), or had undergone liver transplantation (n = 25), 2,149 were potentially eligible for re-engagement, of whom 422 (19.6%) were successfully re-engaged. Significant fibrosis (≥ F2 by FibroScan®) was present in 311 patients (73.7%). Antiviral therapy was initiated in 224 patients, with sofosbuvir/velpatasvir prescribed in 70.1% and glecaprevir/pibrentasvir in 29.9%. SVR12 was achieved in 97.9% of treated patients. In a subset of 112 patients, SVR4 showed 100% concordance with SVR12. In the laboratory cohort, anti-HCV positivity was independently associated with higher all-cause mortality (OR 4.75; 95% CI 3.82–5.94).
Conclusions. Complementary case-finding strategies combined with a simplified two-visit care pathway enabled effective re-engagement and timely treatment, achieving near-universal virologic cure. This scalable model supports hepatitis C micro-elimination across public hospital networks.
References
-1. WHO. Global progress report on HIV, viral hepatitis and sexually transmitted infections, 2021. Geneva: World Health Organization; 2021.
-2. Forns X, Lee SS, Valdes J, et al. Glecaprevir plus pibrentasvir for chronic hepatitis C virus genotype 1, 2, 4, 5, or 6 infection in adults with compensated cirrhosis (EXPEDITION-1): a single-arm, open-label, multicentre phase 3 trial. Lancet Infect Dis. 2017;17(10):1062-1068. DOI:10.1016/S1473-3099(17)30496-6.
-3. Feld JJ, Jacobson IM, Hézode C, et al. Sofosbuvir and velpatasvir for HCV genotype 1, 2, 4, 5, and 6 infection. N Engl J Med. 2015;373(27):2599-2607. DOI:10.1056/NEJMoa1512610.
-4. Liu CH, Liu CJ, Hung CC, et al. Glecaprevir/pibrentasvir for patients with chronic hepatitis C virus infection: real-world effectiveness and safety in Taiwan. Liver Int. 2020;40(4):758-768. DOI:10.1111/liv.14295.
-5. World Health Organization. Combating Hepatitis B and C to Reach Elimination by 2030: Advocacy Brief. Geneva: World Health Organization; 2016.
-6. Polaris Observatory HCV Collaborators. Global prevalence and genotype distribution of hepatitis C virus infection in 2015: a modelling study. Lancet Gastroenterol Hepatol. 2017;2(3):161-176. DOI:10.1016/S2468-1253(16)30181-9.
-7. Marciano S, Haddad L, Borzi SM, et al. Access to direct-acting antivirals for the treatment of hepatitis C in a country with limited resources. Rev Gastroenterol Mex. 2018;83(2):208-211. DOI:10.1016/j.rgmx.2018.02.009.
-8. Safreed-Harmon K, Blach S, Aleman S, et al. The Consensus Hepatitis C Cascade of Care: Standardized Reporting to Monitor Progress Toward Elimination. Clin Infect Dis. 2019;69(12):2218-2227. DOI:10.1093/cid/ciz714.
-9. Mendizabal M, Thompson M, Gonzalez-Ballerga E, et al. Implementation of a re-linkage to care strategy in patients with chronic hepatitis C who were lost to follow-up in Latin America. J Viral Hepat. 2023;30(1):56-63. DOI:10.1111/jvh.13758.
-10. van Dijk M, Drenth JPH; HepNed study group. Loss to follow-up in the hepatitis C care cascade: a substantial problem but opportunity for micro-elimination. J Viral Hepat. 2020;27(12):1270-1283. DOI:10.1111/jvh.13399.
-11. Roblero JP, Arab JP, Mezzano G, Mendizabal M. Hepatitis C virus infection: What are we currently doing in Latin America about WHO's proposals for 2030? Clin Liver Dis (Hoboken). 2021;18(2):72-75. DOI:10.1002/cld.1084.
-12. Ferraz MLG, Andrade ARCF, Pereira GHS, et al. Retrieval of HCV patients lost to follow-up as a strategy for hepatitis C micro-elimination: results of a Brazilian multicentre study. BMC Infect Dis. 2023;23:468. DOI:10.1186/s12879-023-08169-0.
-13. Chen CJ, Huang YH, Hsu CW, et al. Hepatitis C micro-elimination through the retrieval strategy of patients lost to follow-up. BMC Gastroenterol. 2023;23(1):40. DOI:10.1186/s12876-023-02665-y.
-14. Heil J, Soufidi K, Stals F, et al. Retrieval and re-evaluation of previously diagnosed chronic hepatitis C infections lost to medical follow-up in the Netherlands. Eur J Gastroenterol Hepatol. 2020;32(7):851-856. DOI:10.1097/MEG.0000000000001593.
-15. Isfordink CJ, van Dijk M, Brakenhoff SM, et al. Hepatitis C elimination in the Netherlands (CELINE): how nationwide retrieval of lost-to-follow-up hepatitis C patients contributes to micro-elimination. Eur J Intern Med. 2022;101:93-97. DOI:10.1016/j.ejim.2022.04.024.
-16. Overton K, Clegg J, Pekin F, Wood J, McGrath C, Lloyd A, et al. Outcomes of a nurse-led model of care for hepatitis C assessment and treatment with direct-acting antivirals in the custodial setting. Int J Drug Policy. 2019;72:123-128. DOI:10.1016/j.drugpo.2019.02.013.
-17. Papaluca T, McDonald L, Craigie A, Gibson A, Desmond P, Wong D, et al. Outcomes of treatment for hepatitis C in prisoners using a nurse-led, statewide model of care. J Hepatol. 2019;70(5):839-846. DOI:10.1016/j.jhep.2019.01.012.
-18. Ridruejo E, Soza A. Which strategies should be implemented in Latin America to eradicate hepatitis C virus by 2030? Clin Liver Dis (Hoboken). 2019;13(2):43-45. DOI:10.1002/cld.771.
-19. Rubinstein A, Zerbino MC, Cejas C, López A. Making universal health care effective in Argentina: A blueprint for reform. Health Syst Reform. 2018;4(3):203-213. DOI:10.1080/23288604.2018.1477537.
-20. Sotera GF, Ferreiro M, Martes M, et al. Revinculación de pacientes con hepatitis C en el contexto de COVID-19. Acta Gastroenterol Latinoam. 2022;52(1):64-70. DOI:10.52787/agl.v52i1.180.
-21. Ministerio de Salud de la Nación. Boletín Nº 6 | Hepatitis virales en la Argentina. Año VI - Julio 2024. Dirección de Respuesta al VIH, ITS, Hepatitis Virales y Tuberculosis.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 Fernando Cairo, Nicolás Domínguez, Andrea Curia, Lucía Navarro, Manuel Barbero, Ayelen Trillo, Daniel Calfunao, Rodrigo Belloni, Anselmo Adrián Bologna, Estefanía Burgos, Melina Susana, Silvia Mabel Borzi, Omar Andrés Galdame, Esteban González Ballerga, Ignacio Roca

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









